All published articles of this journal are available on ScienceDirect.

Customized Subperiosteal Dental Implants: A State-of-the-Art Narrative Review
Authors Info & Affiliations
Abstract
Objective
This state-of-the-art review aims to consolidate current clinical knowledge, emerging technologies, and evolving applications of customized subperiosteal dental implants for jaw reconstruction in patients with severe atrophic jaws.
Background
Although historically abandoned due to high failure rates, subperiosteal implants have re-emerged as a viable graftless solution, driven by advances in digital workflows, implant design, and biomaterial technology.
Methods
A focused literature search was conducted in June 2025 using PubMed, Scopus, Web of Science, and Google Scholar to identify relevant case reports, case series, and reviews. As this is a narrative review, no quality assessment or meta-analysis was performed.
Results
Contemporary subperiosteal implants, fabricated using CBCT, CAD/CAM, and 3D printing technologies, demonstrate excellent bone adaptation, favorable biomechanics, and 5-year survival rates exceeding 90%. However, the available evidence is primarily derived from low-to-moderate certainty sources. Recent innovations include the use of titanium or PEEK frameworks, bioactive surface modifications, and immediate loading protocols. Primary indications include Cawood–Howell class V–VIII atrophy, failed bone grafts, and medically compromised patients. Contraindications comprise poor oral hygiene and uncontrolled systemic disease.
Discussion
Customized subperiosteal implants are a promising graftless solution for severe atrophy; however, higher-level long-term evidence is still required to confirm their efficacy and safety.
Conclusion
Customized subperiosteal implants represent a promising digital approach for the rehabilitation of complex atrophic jaws. While high-level evidence remains limited, this narrative review highlights their expanding clinical applications and identifies key areas requiring future systematic investigation.
1. INTRODUCTION
Subperiosteal dental implants have gained significance in the field of innovative implant dentistry, especially for patients who show extreme alveolar bone loss, for whom it is impossible for endosseous implants to do any work in their presence. The idea of subperiosteal dental implants came from the mid of the 20th century, which helped in replacing these with innovative materials, inaccuracies of manufacturing processes, and titanium alloys, therefore eventually leading to their sidetracking for the development of osseointegrated endosteal implants and bone augmentation surgeries [1, 2].
However, interest in customized subperiosteal implants is gaining momentum once again with the advent of digital dentistry systems such as cone beam computed tomography, computer-aided design and computer-aided manufacturing, and additive manufacturing in the previous decade [1-4]. This was achieved by the use of customized implants designed according to the morphology of the residual bone.
Improvements in Cone Beam Computed Technology (CBCT) and the finite element analysis of the interaction of the functional components of the implant and the bone, and the development of new biomaterials such as titanium and PEEK, have spurred the development of new implants for the purpose of achieving a better fit and greater biological function [7, 8]. Critically, these implants provide a graftless, single-stage solution for patients with anatomically compromised conditions, with emerging evidence suggesting survival rates exceeding 90% at 5 years [2, 9, 10].
Aside from these advantages, customized implants offer an ideal solution for patients with severely atrophied jaw ridges, as they do not involve grafting procedures [5]. Furthermore, the qualities offered by non-bony customized implants enable one to develop an immediate rigidity in the area of insertion. The rigidity will prove to be valuable to the patient, especially when the health conditions have led to them being medically compromised or when one uses more invasive procedures for rehabilitation [5-7].
As a state-of-the-art narrative review, this paper synthesizes current clinical insights, technological innovations, and evolving indications for customized subperiosteal implants. It aims to contextualize their application within existing reality, specifically in relation to complex cases of presentation that entail severe atrophy, failed reconstruction, or systemic contraindications for bone grafting, within the constraints implicit in an explanatory narrative synthesis. By reviewing their history in relation to a digital solution, there is a clinically focused approach to an ever-quickly advancing horizon related to personalized implant reconstruction.
2. METHODS
This article is a state-of-the-art narrative review and does not follow systematic review methodology (e.g., PRISMA guidelines) or include a formal risk-of-bias assessment. In June 2025, a focused literature search across PubMed, Web of Science, Google Scholar, and Scopus databases was conducted to identify clinically relevant literature on customized subperiosteal dental implants. Search terms included combinations of subperiosteal implant, customized, patient-specific, 3D printing, digital workflow, severe bone atrophy, and CAD/CAM. The focus was on peer-reviewed case series, clinical reports, and recent reviews, published within the last decade, that demonstrate modern indications, digital workflows, and outcomes. However, the selection was based on clinical relevance and representativeness rather than an exhaustive approach. Additionally, quality assessment was not conducted in the study, which was consistent with the narrative review approach. One of the most important points in the narrative review being made here is the important change in clinical indications with time, technologic developments, based on the reality of the world at the time.
2.1. Definition, Evolution & Core Concept
Subperiosteal dental implants are considered to be extraosseous implants, meaning they are placed on the alveolar ridge beneath the periosteum. These implants were specifically for patients with highly atrophied ridges, in whom conventional endosseous implants could not be inserted [2, 9]. Although endosteal implants rely on osseointegration, their maintenance in position within the bone relies on their good adaptation to the ridge. This is in contrast to transosteal implants, in which implants cross the mandible. These implants have largely been abandoned, mostly for high complications (Fig. 1) [2, 9].
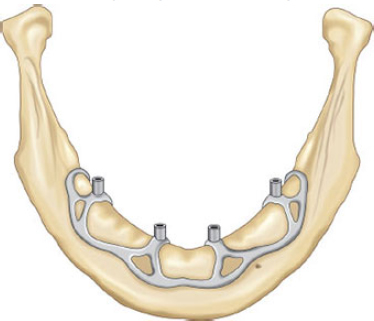
Schematic of a modern customized subperiosteal implant resting on the alveolar ridge beneath the periosteum.
The first ones developed in the 1940s consisted of cobalt-chromium alloy materials with the indirect impression technique. They had ill-fitting, bulky frames with inefficient force distribution. They were shown to have a high failure rate, with survival rates of 12%-26% at 30-35 years due to tissue dehiscence, infections, and framework fractures [2, 3, 10], before becoming less popular with the advent of osseointegrated endosteal appliances and bone grafting in the 1980s.
However, the “digital dentistry” revolution has sparked renewed interest in subperiosteal implants. Furthermore, current subperiosteal implants are customized and fabricated with a precision of not more than a millimeter using CBCT and CAD/3D printing technology [1-4], making casting inaccuracies a thing of the past with today's “digital dentistry.”
FDA-approved implants have now been designed using Finite Element Analysis (FEA), incorporating stress redistribution and strategically placed fixation points on the cortical bone-areas including the nasal spine and external oblique ridge [4, 6].
Materials have also improved. The use of Titanium Alloys, such as Ti-6Al-4V, has become common in the production of implants because of their biocompatibility and other features, such as modifiability based on surface properties. It has a bone-like elastic modulus; however, because it is biologically inert, PEEK also requires surface modifications to enable proper integration with tissue [11-14].
More critically, however, is that contemporary subperiosteal appliances are not simply replicas of those devices from days of yore, since these newer devices are digitally supported, biomechanically superior, and bone augmentation serves no purpose because of immediate or early loading possibilities. Furthermore, these appliances offer a graft-free solution technique in anatomically challenged patients [2, 5, 15].
This transition from working with loosely descriptive systems to precision engineering and individualized devices has led to the subperiosteal implant moving from the last port of call for the practitioner to an effective choice in carefully selected cases when traditional implantology is no longer anatomically indicated.
2.2. Clinical Indications & Contraindications
Customized subperiosteal implants have been considered for severely atrophic alveolar ridges, generally classified as Cawood and Howell V-VIII [2, 16], when bone quantity is insufficient for a standard endosseous implant procedure. Instead, the rationale for these implants is a graftless one-stage solution that does not require bone augmentation.
Key indications include failed prior bone grafts, where regenerative procedures have not achieved adequate bone volume or stability [15, 17-19]. In such cases, subperiosteal frameworks provide immediate structural support by adapting to residual cortical bone, avoiding compromised graft sites.
They are also valuable for patients unsuitable for zygomatic implants, such as those with sinus pathology, unfavorable anatomy, or prior maxillary surgery [20-23]. Unlike zygomatic fixtures that penetrate the sinus, subperiosteal implants distribute occlusal loads across the residual ridge without violating sinus integrity, reducing infection and complication risks.
Patients who have systemic disease that interferes with the body’s ability to heal bones are at increased risk of implant failure. Examples of systemic disease include osteoporosis, prolonged use of corticosteroids, renal osteodystrophy, or treatment with bisphosphonates. For these patients, subperiosteal dental implants may provide an advantage because they rely on mechanical retention instead of osseointegration as a means to retain an implant in place [24]. Patients who receive radiation to the head and neck are presented with bone that is hypoxic and hypovascularized, so the placement of a subperiosteal dental implant in place of an initially endosseous implant would minimize the amount of surgical trauma to the patient and reduce the risk of osteoradionecrosis [9, 25].For subperiosteal implant therapy, a good candidate would be an elderly or medically compromised patient because the surgery is performed as a single-stage procedure with reduced operating time and quicker recovery [26, 27]. Furthermore, patients who must undergo immediate functional rehabilitation, whether through complete edentulousness or experiencing psychosocial distress, would also benefit from the use of immediate or early loading protocols (Table 1) [3, 5, 7].
| Category | Indications | Contraindications |
|---|---|---|
| Bone Conditions | Cawood-Howell classes V–VIII atrophy, failed grafts, irradiated bone | Active oral infections (e.g., untreated periodontitis) |
| Medical Status | Osteoporosis, bisphosphonate use, renal osteodystrophy | Uncontrolled diabetes, immunocompromised states |
| Surgical History | Prior implant failures, oncologic resections | Severe bruxism or parafunctional habits |
| Patient Factors | Elderly patients, urgent prosthetic needs | Poor oral hygiene, unrealistic expectations |
| Anatomic Limitations | Insufficient bone for endosseous implants, sinus complications | Allergies to implant materials (e.g., titanium) |
2.3. Contraindications
Infection in the active state of maxillary region diseases, periodontitis, or periapical diseases predisposing to infection after surgery [9, 28, 29]; there are also absolute contraindications regarding systemic diseases that are at an inappropriate stage of control, like diabetes, immunosuppression, or bleeding disorders, which may predispose complications of healing [9, 30, 31].
Another very important contraindication is poor personal and implant hygiene, as subperiosteal implants require high maintenance. Poor hygiene can result in peri-implant mucositis and bone loss. They should not opt for this procedure, especially when they cannot maintain high standards of hygiene.
Excessive forces associated with severe bruxism or parafunction may produce fatigue, loosening, or fracture of the framework over time [10, 32, 33]. Although occlusal guards may be used to prevent these complications, parafunction that is not controllable is a relative contraindication.
Allergies to materials such as titanium or cobalt-chromium alloys may also need consideration. While PEEK offers a nonmetallic option, the long-term durability of this material when used in subperiosteal implants is still being studied [34].
Insufficiency of keratinized surrounding tissue in the implant site causes instability of the peri-implant soft tissues and an increased risk of mucosal recession and exposure [35-37]. In these situations, soft tissue grafting can sometimes be indicated before or during the time of implant placement.
Finally, unrealistic expectations or complacency among patients can ruin this. The success of rehabilitation work or any other depends on the support of the patients and proper expert maintenance after the surgery [9]. Costs can also be a limitation, as personalized inserts are more expensive due to advanced imaging and production technology [30].
2.4. Digital Workflow
The clinical feasibility of contemporary customized subperiosteal implants relies upon a closed-cycle digital workflow that translates subject anatomy into a precision-crafted prosthetic solution. High-resolution three-dimensional imaging, usually provided by cone beam computed tomography (CBCT), is the first step. By using imaging with CBCT, it is possible to measure the morphology of an alveolar ridge with severe resorption accurately, with results that reach resolutions of a fraction of a millimeter [1-4]. Using CBCT, both soft and hard tissues can be digitally represented; this will be used to produce virtual implants (Fig. 2).
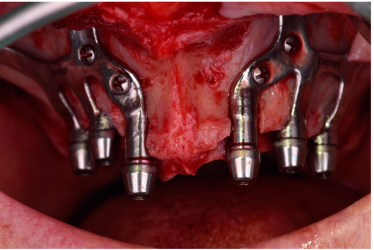
Passive adaptation of a 3D-printed subperiosteal framework to the residual bone surface, ensuring optimal load distribution. Reproduced from [Herce-López et al., Biomimetics, 2024] under the terms and conditions of the Creative Commons Attribution (CC BY) license [15].
Engineers and clinicians can create custom-fit devices using Computer-Aided Design (CAD) software and work closely together to develop patient-specific CAD drawings. CAD drawings contain information about the desired device's specifications (e.g., material type, size) and are used to create an exact match of the remaining bone's topography [1, 15]. CAD removes the problems associated with previous technique impressions, leading to dimensional discrepancies, which ensures a passive or non-moving fit and decreases microscopic movement and discomfort from soft-tissue interference [2, 38]. In addition, Finite Element Analysis (FEA) is regularly utilized during the design stage to replicate function and equalise the distribution of loading throughout the framework [4, 6]. Therefore, the strategic addition of rigid strength to highly stressed areas (e.g., the molar area) and the addition of lightweight lattice structures to areas of low or no load have been achieved to achieve an optimal combination of strength and reduced weight [39, 40].
The final implant product is created through additive manufacturing (3D printing), and this is often carried out through either Selective Laser Melting (SLM) or Electron Beam Melting (EBM) [7, 41, 42]. Both powder bed fusion methods utilize titanium powder to create the implant in a layer-by-layer fashion, thus achieving an architecture that is hard to achieve or even impossible using casting methods [39, 43]. Thus, the end product has a lightweight, solid architecture with biomechanical properties adapted to an individual’s anatomy [2, 44].
Choosing the material is really important for success. Titanium alloys like Ti6Al4V are the choice because they work well with the body, withstand heavy use, and help bone grow around them. Some changes can also be made to the surface of these materials, such as sandblasting or acid-etching, to help them work better with the soft tissues and bones [11-14]. This makes a difference at the point where the implant meets the bone. Titanium alloys like Ti6Al4V remain a viable choice because they offer excellent properties [45, 46]. When an individual has metal allergies or concerns about their appearance, PEEK may be a good alternative because it is radiolucent on X-ray and contains no metal components [8, 34]. While it already is biocompatible, its compatibility with tissue can be improved through surface modification, such as by using a titanium overlay or hydroxyapatite [14, 47]. Ti-6Al-4V titanium alloy, polyetheretherketone or PEEK, for example, represent some of these materials. Its low elastic modulus (~3-4 GPa compared to titanium at ~110 GPa) does help in reducing stress shielding, which might conserve bone in atrophic ridges [48, 49].
A major advancement is the shift toward designing treatment plans with prosthetics as the primary focus. The prosthetic is planned before the framework is fabricated to ensure optimal function and aesthetics. This approach supports ease of maintenance and repair if complications arise. Components such as angled abutments and screw-retained prostheses are incorporated to achieve these goals. Digital smile design is also applied to ensure that the prosthetic is both functional and visually harmonious, which is essential for long-term success. Post-processing techniques continue to enhance clinical outcomes. Electropolishing smooths transmucosal components to reduce plaque accumulation [50-54], and quality control using coordinate measurement machines and micro-CT imaging verifies dimensional accuracy before delivery [55, 56]. With this continuous flow from imaging to implantation, one-stage surgery and immediate/early loading have been achieved with marked efficacy and a remarkably short treatment time and morbidity rate [2, 27]. The need for intraoperative adjustments is also greatly reduced, since it is designed for passive seating without intervention [15, 38].
The future of design optimization is supported by Artificial intelligence using automated methods to design, while Hybrid materials (Titanium-PEEK composites) and Bioactive Coatings have been developed to improve biological integration with implants [57-59]. There is still limited Long-term (>10 Years) data; however, the current information available supports the view that Digital Subperiosteal implant (DSI) technology is a predictable, graftless treatment alternative for the most anatomically damaged patients.
This new technology has changed the perception of DSI from an option for “last resort” patients to a first-line treatment in certain clinical situations (Table 2).
| Property | Titanium (Ti6Al4V) | PEEK (60% CF-Reinforced) | Hydroxyapatite-Coated Titanium |
|---|---|---|---|
| Biocompatibility | Excellent (osseointegration) | Good (no osseoconduction) | Excellent (osteoconductive) |
| Elastic Modulus (GPa) | 100–120 | 3–4 | 100–120 |
| Strength (MPa) | 960–1270 | 150–200 | 960–1270 |
| Corrosion Resistance | High (passive oxide layer) | High | High |
| Manufacturing Method | SLM, EBM | Injection molding, SLM | SLM with post-coating |
| Radiolucency | Opaque | Radiolucent | Opaque |
| Clinical Survival Rate | 97.8% (5 years) | Limited data | >95% (5 years) |
| Key Advantages | Osseointegration, durability | Lightweight, low stress | Enhanced bone bonding |
| Key Limitations | Stress shielding | Poor bone adhesion | Coating delamination risks |
2.5. Surgical Protocol & Outcomes
The position of implants placed by surgeons in Customized Subperiosteal Implantology has been achieved in an optimum, digitally supported way, which has minimized invasiveness, susceptibility to error, and uncertainties. Before carrying out dental implants, preoperative planning, which has used CBCT imaging and intraoral scanning, has enabled a virtual 3-D reconstruction of the atrophied jaw in the patient, acting as a reference for preparing an optimum, Finite Element Analysis-supported, titanium or PEEK framework, with goals of passive fitting of implants for optimum force distribution (Fig. 3) [2, 15, 38].
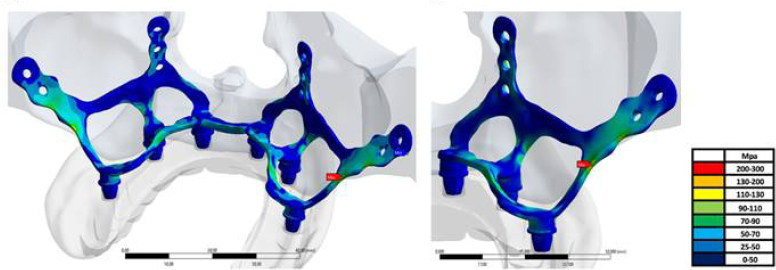
Finite element analysis showing stress distribution across a subperiosteal implant under functional loading. (A) Stress distribution map across the implant framework, showing concentrated forces (red areas) at fixation points and along the posterior struts. (B) Corresponding stress distribution on the underlying cortical bone, indicating physiological load transfer without pathological overloading [Ayhan et al., Biomimetics, 2023] under the terms and conditions of the Creative Commons Attribution (CC BY) license [72].
It is performed by local anesthesia with sedation or general anesthesia based on the patient's condition. A full-thickness mucoperiosteal flap is elevated to fully expose the ridge while exercising care not to damage the periosteum. The custom framework is placed directly on top of the bone without requiring intra-oral repairs, as with modern computerized techniques [15, 38]. To ensure passive adaptation with fixed non-rocking and pressure-point-free adaptation in the final restoration, a pressure test of passive adaptation is needed.
Primary stability is achieved through fixation with 3–6 titanium screws (1.5–2.0 mm diameter) placed in areas of dense cortical bone-such as the nasal spine, zygomatic buttress, or mandibular symphysis-based on preoperative planning [15, 38]. This screw-retained design prevents micromotion, which is critical for soft tissue integration and long-term success. The transmucosal abutments are positioned to allow optimal prosthetic emergence and hygiene access.
Flap closure is performed tension-free, often with periosteal releasing incisions or advancement techniques to ensure complete coverage of the framework. Inadequate soft tissue management is a leading cause of early wound dehiscence and framework exposure [60]. Postoperatively, patients receive antibiotic prophylaxis, anti-inflammatory medication, and chlorhexidine rinses, and are instructed to follow a soft diet for 4–6 weeks.
The important benefit associated with this technique is the possibility of early loading. In most instances, the provisional implant support is placed in 24-72 hours, and there is immediate function and psychological benefit-especially for senior and cancer patients [2, 27, 44]. The definitive support is placed 3-6 months after the procedure when the soft tissue has matured.
Outcome results have also been very encouraging. Recently published articles revealed that the 5-year survival rate of the subperiosteal implants created with digital technology was above 90% [2, 9, 61]. A multi-center clinical trial showed a 95% survival rate at 3 years in 68 patients with severe maxillary atrophy [62]. However, it is important to note that the aforementioned results differ significantly from those of previous subperiosteal implants, which failed by 50-70% at 10-15 years due to poor adaptation and infection [10].
Success is achieved by careful patient selection, digital accuracy, and soft tissue management. Failure is usually attributed to lack of cleanliness, uncontrolled systemic disease, or a lack of keratinized tissues, and not a function of the design of the osseointegrative system itself. Although there is a limited follow-up period past the ten-year mark on most current systems, there is merit to a customized subperiosteal approach that is predictable without the need for bone-grafting augmentation when applied to an anatomically compromised patient base through a comprehensive digital and clinical approach (Table 3 and Fig. 4).
| Study (Year) | Number of Implants / Patients | Follow-Up Duration | Success / Survival Rate |
|---|---|---|---|
| Mangano et al. (2020) [1] | 6 implants / 4 patients | 12 months | 100% |
| Łoginoff et al. (2024) [2] | 31 implants / 28 patients | 36 months | 96.8% |
| Van Den Borre et al. (2025) [19] | 15 implants / 15 patients | 24-60 months | 100% |
| Vaira et al. (2024) [25] | 45 implants / 39 patients | 36 months | 97.8% |
| Onică et al. (2024) [44] | 20 implants / 18 patients | 6 years | 95% |
| Anitua et al. (2024) [9] | 312 implants (from multiple studies) | 12-60 months | 94.9% |
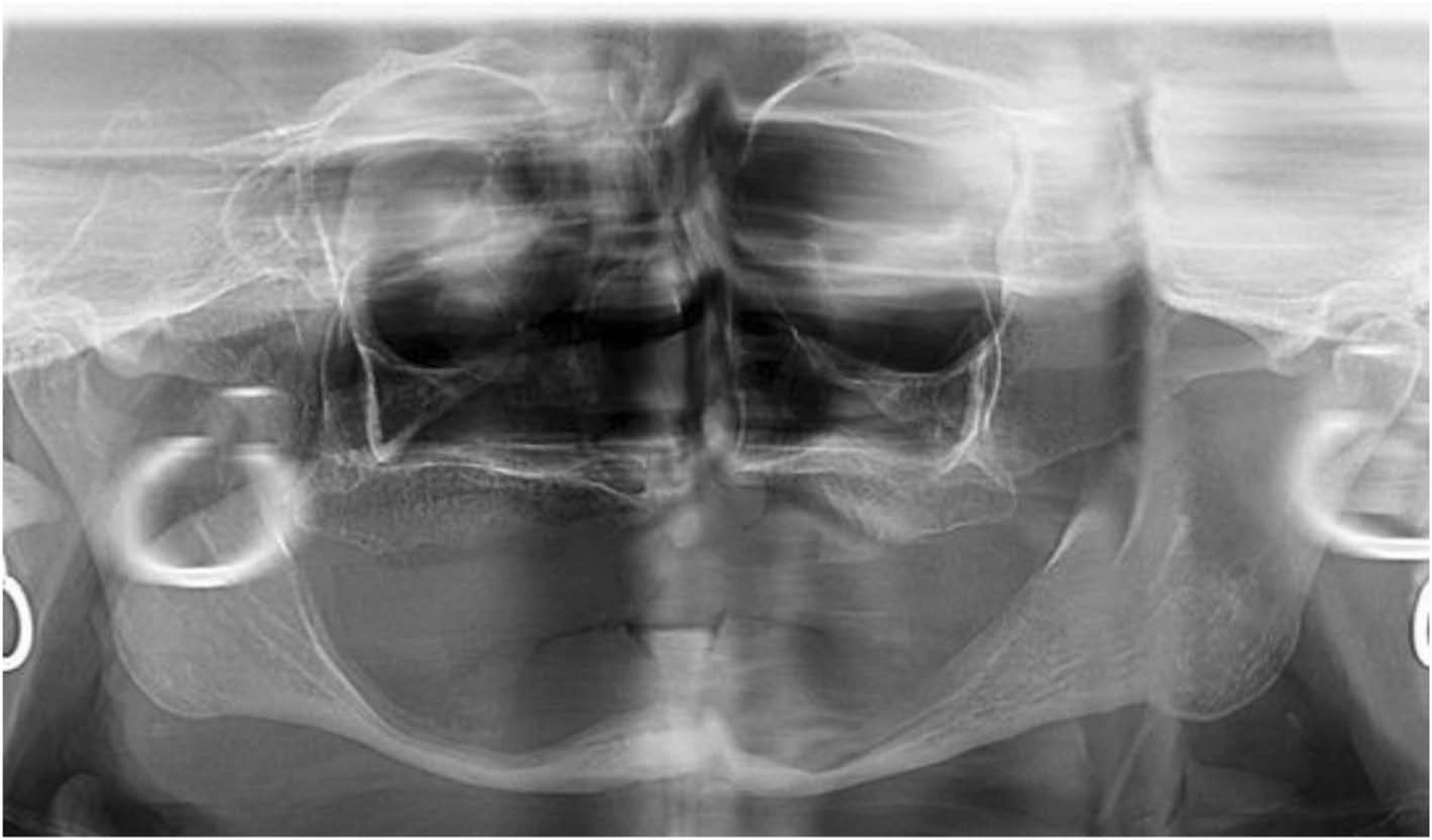
Linical application of customized subperiosteal implants in a patient with Cawood–Howell class VII maxillary atrophy, demonstrating digital planning, surgical placement, and final prosthetic rehabilitation. Preoperative cone-beam computed tomography (CBCT)–based 3D reconstruction showing severe maxillary atrophy (Cawood–Howell class VII) with minimal residual bone height. Reproduced from [Filipov et al., Head Face Med, 2021] under the terms and conditions of the Creative Commons Attribution (CC BY) license [70].
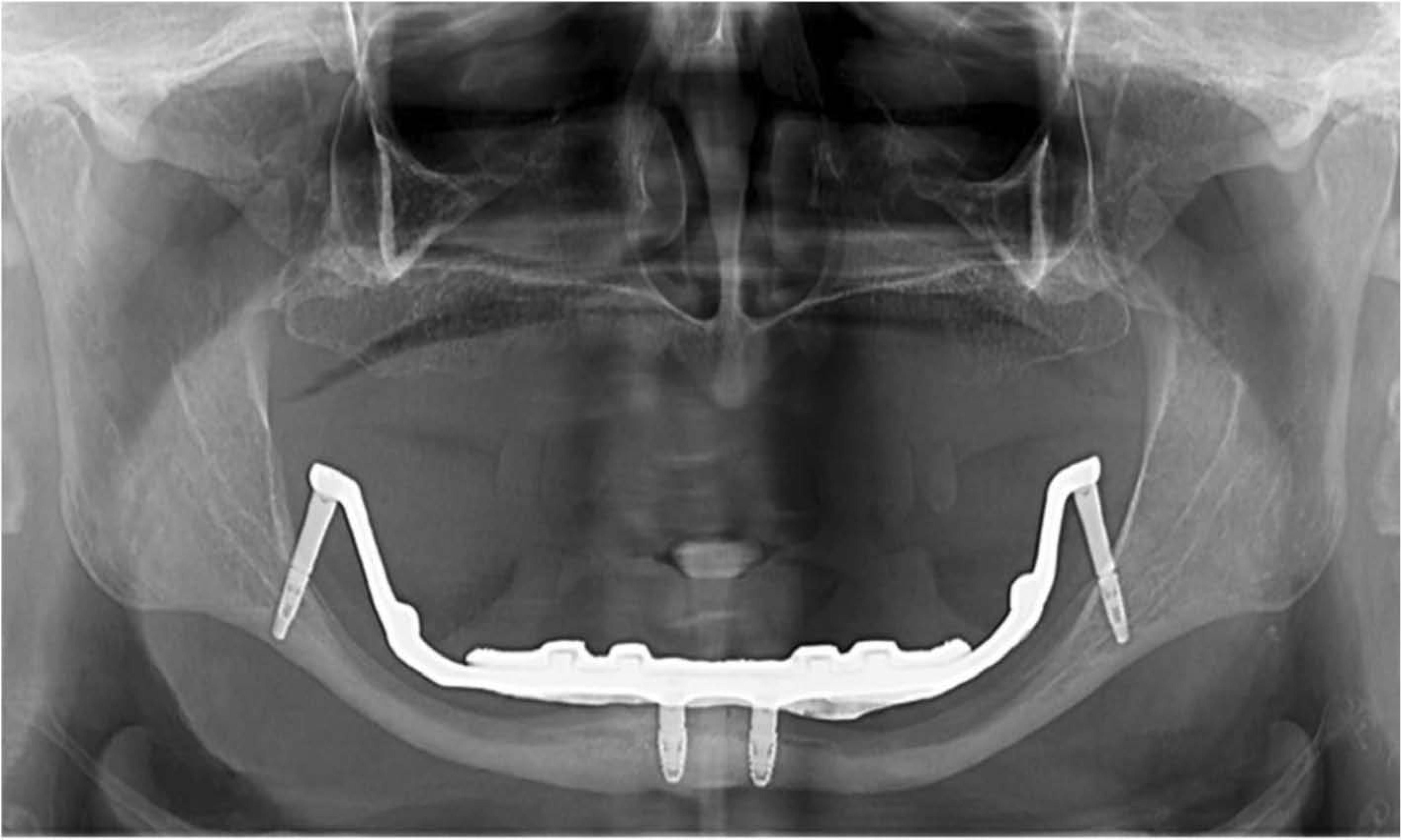
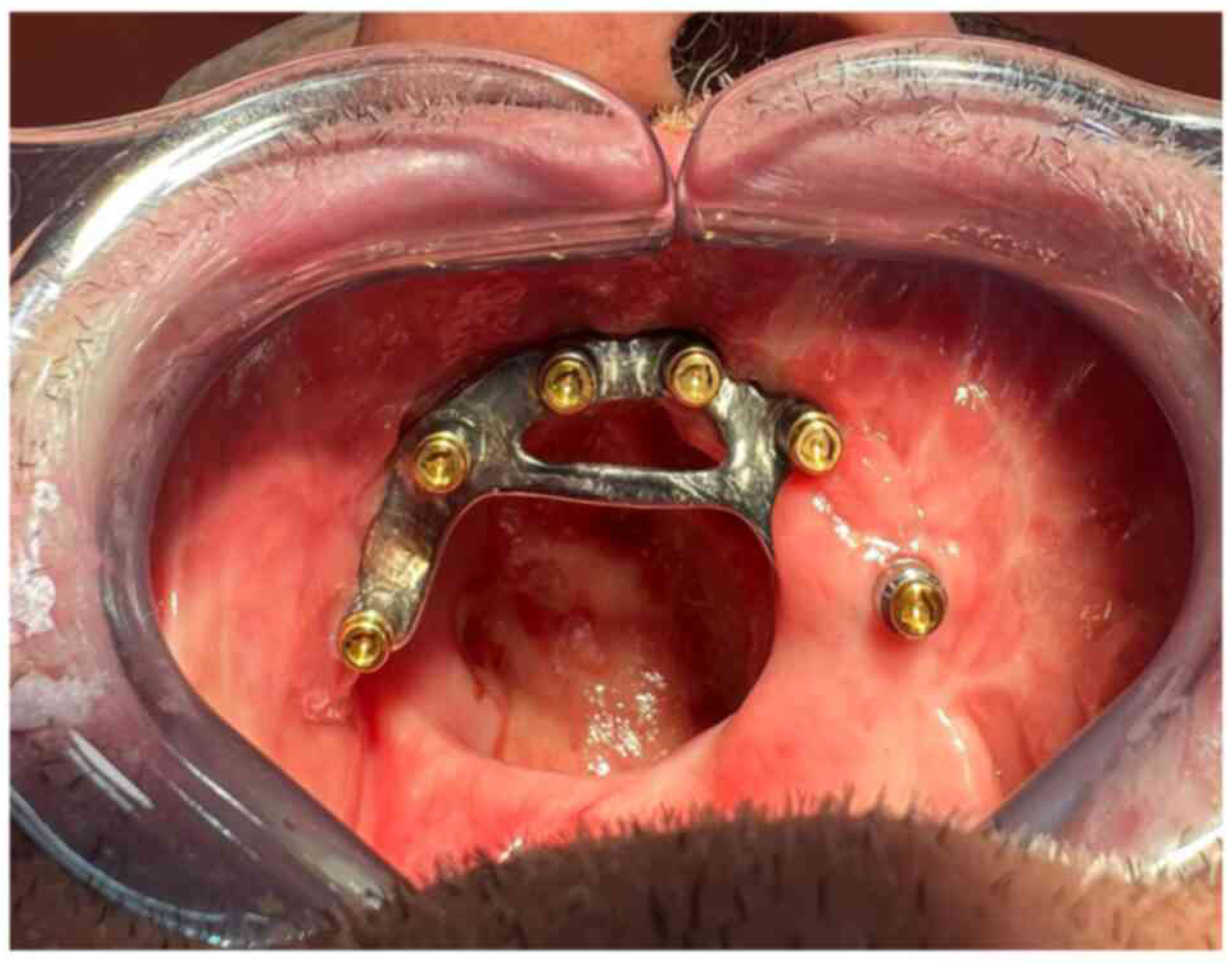
Intraoperative view of the passive fit of the 3D-printed titanium subperiosteal framework seated directly onto the residual alveolar ridge, secured with fixation screws in dense cortical areas. Reproduced from [Filipov et al., Head Face Med, 2021] under the terms and conditions of the Creative Commons Attribution (CC BY) license [70].
Postoperative clinical outcome following prosthetic loading, showing a functional and esthetically pleasing full-arch fixed restoration supported by the customized subperiosteal implant. Reproduced from [Parras‑Hernández et al., Exp Ther Med, 2024] under the terms and conditions of the Creative Commons Attribution (CC BY) license [71].
2.6. Complications
Though there have been immense advances regarding the design, as well as digital fabrication methods, customized subperiosteal implants are also known for their particular spectrum of complications, which require an active method for their management. Dehiscence of soft tissue is the most frequent one and has been identified to have occurrences up to 25.6% among patients, which often leads to partial exposure of the framework [9, 63]. In particular, this happens due to improper flap harvesting, primary closure with tension, and/or the absence of keratinized tissue within the area where the implant is positioned [60].
Peri-implant infection, in relation to the global prevalence, has an incidence of 5.3% [9]. Peri-implant infection in relation to endosteal implants leads to the bone-implant interface being damaged or compromised. Peri-implant infection in relation to subperiosteal implants leads to bone-framework interface compromise, in combination with transmucosal abutment. Due to the complexity of the framework design, it becomes easier for bacteria to colonize the implants, leading to poor hygiene maintenance. The primary treatment for this condition involves mechanical debridement, antibiotic therapy, and strict oral hygiene practices. In advanced cases, surgical maintenance of hygiene around the framework might be considered, whereas in severely advanced cases, implants may need to be removed [30, 64].
Proximal bone resorption under the implant may impair long-term stability. Since subperiosteal implants are retained by mechanical fixation rather than osseointegration, disuse atrophy or inflammation from micromotion may impair bone stability and induce mobility [10]. Using 3-6 titanium screws for stable fixation in dense bony areas (such as the nasal spine and mandibular symphysis) reduces the risk of mobility [15, 38]. In cases where mobility occurs either by losing fixation of the initial titanium screws or due to the continued need for additional screws, it is acceptable to use a different type of implant or to re-fixate using another method. However, with extensive bone loss, it is typically necessary to remove the implant in order to stop the mobility.
Technical complications with the implants occur less often; nonetheless, they are still of importance. An infrequently seen complication of producing a fracture of the framework occurs from fatigue failure in the location of the framework under the load of stress or when patients have bruxism that is not controlled [63]. Contemporary design involves the use of Finite Element Analysis (FEA) to minimize stress concentrations [60]. The majority of prosthetic complications (screw loosening and breakage/ malfunction of provisional-prosthesis) occur at a rate of approximately 5.2%. The majority of prosthetic complications can be rectified through chair-side adjustments or replacement of prosthetic components.
The most critical factor remains prevention. The selection of patients must be made very carefully to exclude patients who have bad oral hygiene, uncontrolled diabetes, and/or unrealistic expectations to minimize biologic risks [9, 31]. The evaluation and augmentation of soft tissue prior to surgery, when indicated, can also enhance the durability of the mucosal tissue. Digital planning is essential for passive fitting and optimal screw positioning, thereby reducing surgical trauma.
However, if complications occur, a stepwise and conservative method should be followed:
- Non-surgical: debridement, antibiotics, occlusal adjustment.
- Surgical: soft tissue grafting, framework modification, or re-fixation.
- Definitive: explantation and transition to alternative rehabilitation (e.g., zygomatic implants or grafting) only when salvage is unfeasible [30].
Most significant complications can be avoided or managed with appropriate case selection, precise execution, and diligent maintenance of the reconstruction; thus, functional and aesthetic advantages of this graft-free solution for severely atrophic jaws can be safeguarded.
2.7. Future Directions & Clinical Perspective
Customized subperiosteal implants are transforming a salvage procedure to a mainstream modality for advanced alveolar atrophy without grafting. The future of customized subperiosteal implants lies with greater integration of artificial intelligence and biomimetics. AI platforms are now being used to automate framework optimization with respect to load distribution and stress concentrations [59, 65].
There are also rapid developments in the field of material science. Bioactive coatings such as hydroxyapatite, titanium plasma spray, and peptide-functionalized coatings are now being developed to promote soft tissue sealing and bone apposition at the implant/tissue interface, which may enable partial osseointegration in the future [46, 57, 58, 66]. Hybrid materials, such as titanium-PEEK composites, are being developed to combine the osseointegration properties of metals with the shock-absorbing qualities of polymers [58].
The potential use of resorbable or bioresorbable scaffolds as temporary mechanical supports to promote bone formation is another exciting area of investigation. These scaffolds can provide mechanical support and allow some degree of resorption, thereby promoting bone formation; therefore, in many instances, they can eliminate the need for a permanent implant [67, 68]. On the other hand, robotic surgery may soon improve the precision of object placement, particularly in complicated cases [69].
From a clinical standpoint, these implants are gradually transitioning from a ‘last resort’ to a first choice for Cawood-Howell Class V to VIII atrophy or in medically compromised or failed grafts. The ability of these implants to be loaded in a single stage meets contemporary expectations of efficiency, predictability, and patient-centered care.
The current 5-year survival rate is higher than 90% [9, 61], but there is little evidence of anything more than a single 10-year follow-up. Multinational registries and comparative studies must be conducted to enable large patient populations with orbitally complex abnormalities to utilize this new operative technique and document its effectiveness compared with traditional methods (e.g., grafting, zygomatic-based reconstruction).
CONCLUSION
Customized subperiosteal implants provide a predictable solution without the need for bone grafting when no other suitable alternatives exist, such as endosteally placed dental implants. These implants also have increased clinical value in difficult circumstances, such as Cawood and Howell classes V, VI, VII, and VIII (severe atrophy); failure of a bone graft; and poor health/medical conditions that do not allow for standard implant protocols. Although this synthesis may not offer any significant evidence, it highlights the fact that customized subperiosteal implant technology is continuing to develop into one of the most valuable tools in dentistry and should be viewed as a first-line option rather than a last resort.
Customized subperiosteal implants offer an effective means of treating severe atrophy based upon the parameters listed above. The development of 3D-printed implants will provide a better fit and help reduce complications such as tissue dehiscence and peri-implant infections. As digital dentistry advances, the number of customized subperiosteal dental implant designs will continue to increase exponentially and will offer a new level of dental treatment to patients who were previously considered untreatable.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: Z.A. and A.K.: Conceived and designed the study; Z.A. and I.B.: Collected the data; Z.A., I.B., and W.K.: Analyzed and interpreted the results; and Z.A. and G.H.: Prepared the draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| AI | = Artificial Intelligence |
| CAD | = Computer-Aided Design |
| CAM | = Computer-Aided Manufacturing |
| CBCT | = Cone-Beam Computed Tomography |
| CMM | = Coordinate Measuring Machine |
| CNC | = Computer Numerical Control |
| DSD | = Digital Smile Design |
| EBM | = Electron Beam Melting |
| FEA | = Finite Element Analysis |
| HA | = Hydroxyapatite |
| PEEK | = Polyetheretherketone |
| SLA | = Sandblasting, Large-grit, Acid-etching |
| SLM | = Selective Laser Melting |
| 3D | = Three-Dimensional |
ACKNOWLEDGEMENTS
Declared none.

