All published articles of this journal are available on ScienceDirect.

Comparative Evaluation of Root Resorption in First Upper Premolars Treated with Active and Passive Self-ligating Brackets: A Prospective Split-mouth Study
Authors Info & Affiliations
Abstract
Introduction
This prospective observational split-mouth study aimed to compare the effect of self-ligating bracket type (active versus passive) on the extent of Orthodontically Induced Inflammatory Root Resorption (OIIRR) in maxillary first premolars during alignment, leveling, and initial torque expression in orthodontic treatment.
Materials and Methods
A split-mouth design was employed in 10 patients (7 females, 3 males; 20 maxillary first premolars). Each patient received simultaneous orthodontic treatment with active and passive self-ligating brackets. The right side was randomly assigned to active self-ligating brackets (Forestadent, Pforzheim, Germany), and the contralateral side to passive self-ligating brackets of the same manufacturer. After nine months, both premolars were extracted and analyzed using a 3D Confocal Laser Scanning Microscope (Lext OLS 4000, Olympus Corporation). Volumetric measurements of resorption craters (area, volume, and depth) were obtained with specialized software.
Results
No statistically significant differences were observed in the extent of external root resorption between active and passive self-ligating brackets. Both bracket systems showed comparable mean values for resorption area, volume, and depth.
Discussion
This study provides the first direct intra-patient comparison of active versus passive self-ligating brackets, eliminating inter-individual variability. Findings suggest that the biological response leading to OIIRR is comparable between both bracket systems, indicating that individual biological susceptibility may outweigh the mechanical differences in bracket clip design during the initial stages of treatment.
Conclusion
Passive and active self-ligating brackets produce comparable levels of orthodontically induced inflammatory root resorption during early stages of treatment. Orthodontic forces should be maintained at the lowest biologically acceptable levels to minimize iatrogenic effects.
1. INTRODUCTION
Orthodontically Induced Inflammatory Root Resorption (OIIRR) remains one of the most significant iatrogenic consequences of orthodontic treatment, characterized by the complex morphological and chemical degradation of root cementum [1-3]. When this resorptive process penetrates the cementum and involves the underlying dentin, the reparative capacity of the tissue is significantly compromised. This imbalance between clastic activity and tissue repair often results in a permanent and clinically relevant loss of root structure [4, 5].
The etiology of external root resorption is multifactorial, involving a complex interplay of patient-related variables such as genetic predisposition, age, sex, and systemic health [4, 6, 7], as well as local factors including dental morphology, previous trauma [8, 9], and periodontal status [10]. Furthermore, occlusal factors and dentoalveolar morphology play a critical role in individual susceptibility [11, 12]. Beyond these biological traits, attention must be directed toward appliance-related variables, specifically the magnitude, duration, and direction of the applied orthodontic forces [5, 13, 14]. Studying these factors through contemporary evidence allows for a clearer understanding of how modern orthodontic appliances influence the tissues and biology of the supporting periodontium [1-3].
Self-ligating brackets represent a major advancement in contemporary orthodontics in terms of design, biomechanics, and clinical efficiency. These systems employ a clip or sliding mechanism to secure the archwire in place [15, 16]. Passive self-ligating brackets act as rigid tubes that retain the archwire, theoretically allowing tooth movement through light, physiologic forces [17]. In contrast, active self-ligating brackets use an elastic clip that exerts pressure on the archwire, storing and releasing energy during elastic deformation [16-20].
2. MATERIALS AND METHODS
A total of 20 maxillary first premolars from 10 patients (7 females and 3 males; mean chronological age: 15.4 years) requiring bilateral extractions as part of their orthodontic treatment were included in this study. The unequal distribution between female and male participants resulted from the strict inclusion criteria and the limited number of patients who met the requirement for bilateral premolar extraction during the recruitment period. Because the study followed a split-mouth design, each patient simultaneously received both bracket systems and therefore served as their own biological control, minimizing potential confounding effects related to sex. Current evidence indicates that sex-related variations in short-term Orthodontically Induced Inflammatory Root Resorption (OIIRR) are generally small and inconsistent, and thus unlikely to influence the primary outcome of this study.
This prospective observational split-mouth study included 10 patients. The sample size was determined based on previous studies evaluating root resorption associated with self-ligating brackets, aiming to detect a clinically significant difference between groups with a statistical power of 80% at a significance level of 5%. The number of patients was considered adequate to address the primary outcome of the study. The study was conducted between 2011 and 2016.
Ethical approval was granted by the Institutional Health Research Ethics Committee (CIEIS) of the School of Dentistry, National University of Córdoba, and authorization was obtained from the Council of Ethical Evaluation of Research (CoEIS), Ministry of Health of Córdoba Province, Argentina (Approval Number: V.1.2011). All patients and their parents/guardians received both verbal and written explanations of the study and provided informed consent prior to participation. All procedures performed in this study involving human participants complied with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
2.1. Inclusion Criteria
(1) Presence of full permanent dentition
(2) Less than 5 mm of dentoalveolar discrepancy
(3) Indication for the extraction of maxillary first premolars to correct skeletal or dental Class II discrepancies
(4) Complete root apexification
(5) Good periodontal health
2.2. Exclusion Criteria
Patients were excluded if they met any of the following criteria:
(1) Upper dental crowding greater than 5 mm, in which immediate extractions would be required prior to bracket placement to avoid damage to supporting tissues
(2) Use of medications or substances that could influence orthodontic tooth movement (e.g., corticosteroids, bisphosphonates, NSAIDs)
(3) History of previous orthodontic treatment
(4) Signs or symptoms of periodontal disease
(5) Signs or symptoms of bruxism
(6) History of dental trauma
(7) Previous endodontic treatment on the teeth to be analyzed
(8) Root dilaceration of the tooth scheduled for extraction
(9) Radiographic evidence of pre-existing root resorption before orthodontic treatment
Before initiating treatment, standard orthodontic records were collected for all patients, including extraoral and intraoral photographs, panoramic and lateral cephalometric radiographs, study casts, and periapical radiographs of the maxillary first premolars.
A split-mouth design was employed. Each patient received both active and passive self-ligating bracket systems simultaneously. The right side was randomly assigned to active self-ligating brackets (Forestadent, Pforzheim, Germany; Roth Prescription), and the left side received passive self-ligating brackets from the same manufacturer and prescription. Thermoactive NiTi archwires (Forestadent, Germany) were placed sequentially according to the manufacturer’s recommendations (0.014, 0.016 × 0.022, and 0.019 × 0.025 inches) until initial torque expression was achieved.
The 0.019 × 0.025-inch wire was maintained for four months to ensure torque expression. Subsequently, the maxillary first premolars were atraumatically extracted from both sides (Fig. 1).
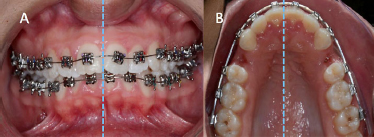
A) Active semi-ligating brackets cemented on the right quadrants and passive self-ligating brackets cemented on the left quadrants. B) Extracted first right and left premolars.
Immediately after extraction, the teeth were sterilized and stored in individual containers with sterile deionized water (Milli-Q; Millipore, Bedford, MA) at room temperature (23°C) until analysis. All samples were examined using a 3D Confocal Laser Scanning Microscope (Lext OLS 4000, Olympus Corporation) at the LAMARX Laboratory, School of Mathematics, Astronomy, and Physics (FAMAF), UNC.
The microscope software enabled quantification of the surface area, width, length, volume, and depth of the resorption craters (Fig. 2). Each root surface (buccal, palatal, mesial, distal) was divided into cervical, middle, and apical thirds for systematic evaluation (Fig. 3). The total resorption area was calculated as the sum of resorption across all thirds. Depth measurements were used to determine whether resorption had extended into the dentin.
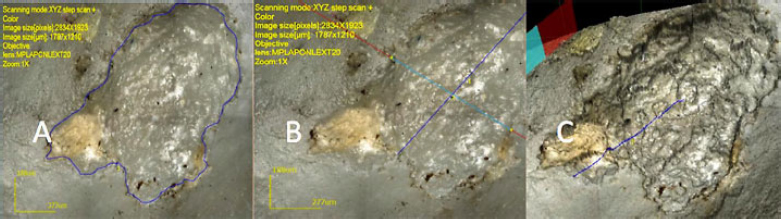
Images from a Confocal Microscope. Measurements: A) Surface Area, B) Length and width, C) Depth.
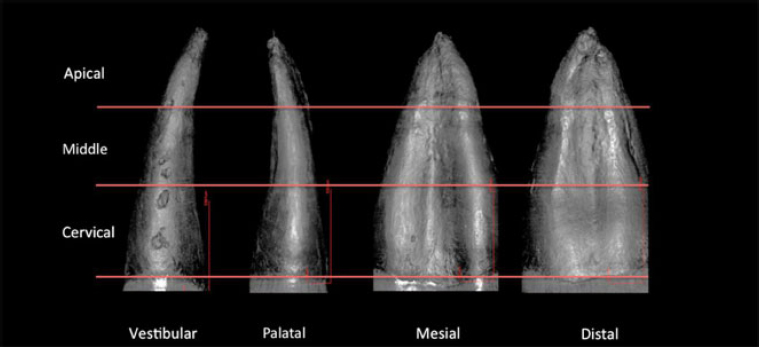
Image from a confocal microscope: Root zones divided into three thirds for systematic analysis. Resorption areas of craters can be seen on the different sides and thirds of the roots.
2.3. Statistical Analysis
Descriptive statistics were calculated for all measured variables (surface area, volume, and depth of resorption). Results are presented as mean ± Standard Deviation (SD) and range. Data distributions were visually inspected using box plots.
Between-group comparisons (active vs. passive self-ligating brackets) were performed using the Wilcoxon signed-rank test for paired samples. For comparisons involving more than two groups (i.e., the different root thirds), the Kruskal–Wallis test was used. When the Kruskal–Wallis test indicated significant differences, two-tailed post hoc multiple comparisons were applied. The threshold for statistical significance was set at α = 0.05.
Correlation analyses were performed to evaluate the relationship between resorption in paired premolars from the same patient, considering both surface area and volume. Additionally, a group-specific analysis was conducted to determine the percentage of resorption lesions that extended beyond the cementum into the dentin.
3. RESULTS
From the original 284 patients screened, 10 met the inclusion criteria. A total of 20 extracted premolars (10 right and 10 left) were analyzed (Fig. 4).
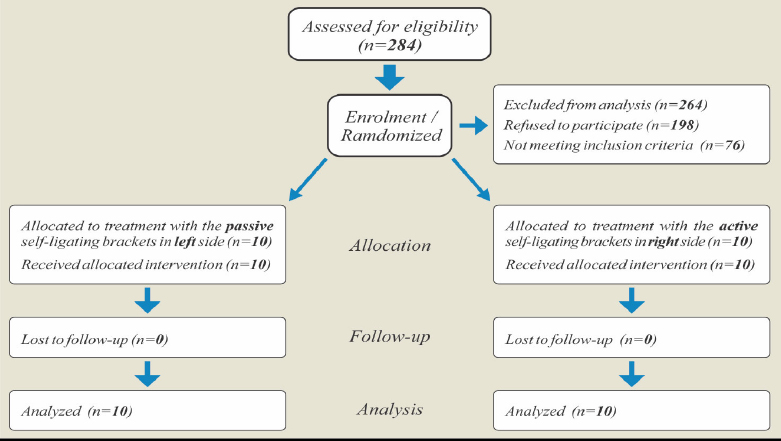
Flow diagram of patients through the study.
In total, 85 resorption sites were identified in the active bracket group and 83 sites in the passive bracket group.
Comparative analysis revealed no statistically significant differences between active and passive self-ligating systems in total external root resorption for surface area (all p-value > 0.05; Fig. 5; Tables 1 and 2), volume (all p-value > 0.05; Fig. 6; Tables 3 and 4), or overall depth (all p-value > 0.05; Fig. 7; Tables 5 and 6).
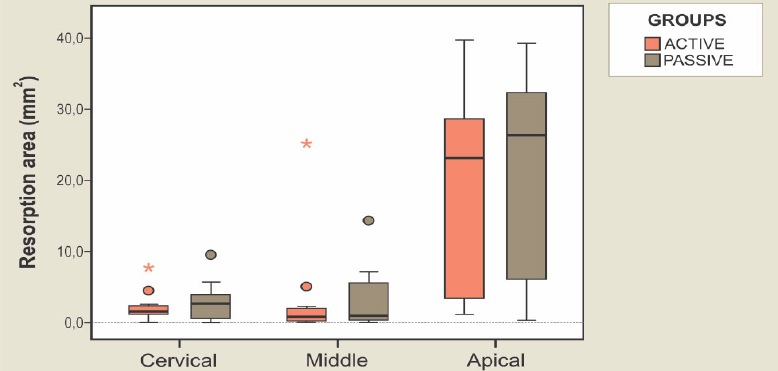
Box plot with the distributions of the values of the resorption area in accordance with each group (active or passive self-ligating brackets, based on each root third). The central lines of the boxes represent the median values; the boxes themselves represent 50% of the more central values of each subgroup; the circles are atypical values and the asterisks represent the extreme values in each subgroup.
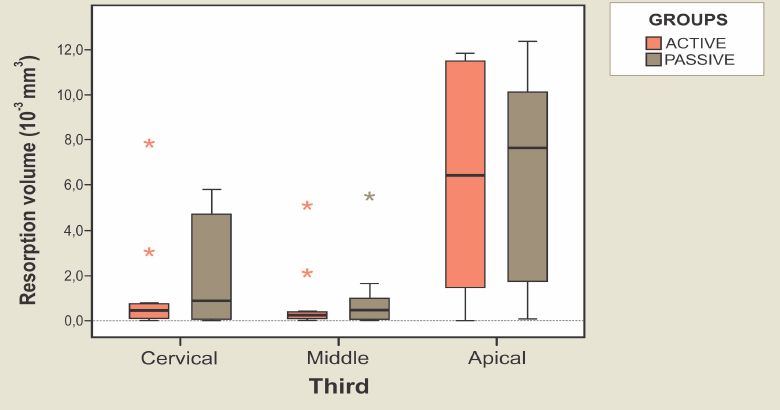
Box plot with the distributions of the values of the resorption volume in accordance with each group (active or passive self-ligating brackets, in accordance with each root third). The central lines of the boxes represent the median values; the boxes themselves represent 50% of the more central values of each subgroup; the circles are atypical values and the asterisks represent the extreme values in each subgroup.
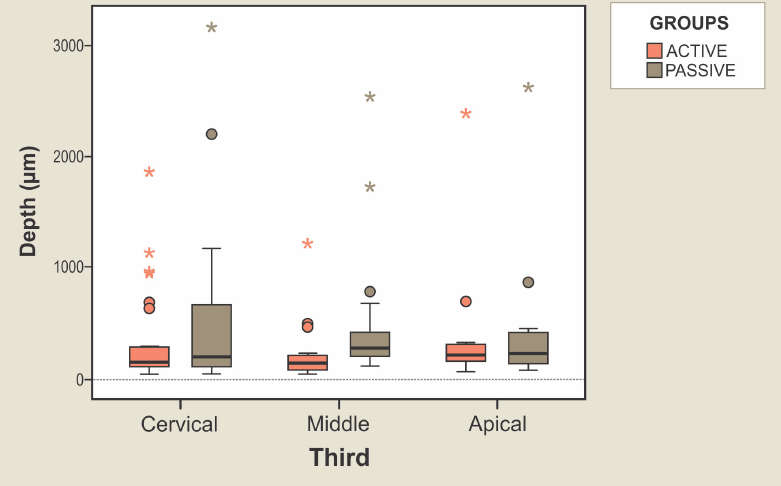
Box plot with the distributions of the values of the resorption depth in accordance with each group (active or passive self-ligating brackets, in accordance with each root third). The central lines of the boxes represent the median values; the boxes themselves represent 50% of the more central values of each subgroup; the circles are atypical values and the asterisks represent the extreme values in each subgroup.
| Third | Active Brackets | Passive Brackets | Sig. (p-value) |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Min. | Max. | Median | SE | SD | Min. | Max. | Median | SE | SD | ||
| Cervical | 0,00 | 7,80 | 2,26 | 0,73 | 2,3 | 0,00 | 9,68 | 3,07 | 0,92 | 2,9 | 0,333 |
| Middle | 0,08 | 25,24 | 3,63 | 2,45 | 7,7 | 0,00 | 14,42 | 3,22 | 1,47 | 4,6 | 0,646 |
| Apical | 0,00 | 39,67 | 19,70 | 4,67 | 14,8 | 0,31 | 39,29 | 20,66 | 4,61 | 14,6 | 0,333 |
| Total | 2,53 | 64,92 | 25,59 | 6,18 | 19,6 | 1,65 | 46,91 | 26,94 | 5,32 | 16,8 | 0,285 |
Note: Values are expressed in mm2.
| Third | Active Brackets | Sig. (p-value) |
Passive Brackets | Sig. (p-value) |
||||
|---|---|---|---|---|---|---|---|---|
| Median | SE | SD | Median | SE | SD | |||
| Cervical | 2,26 | 0,73 | 2,3 | 0,008 | 3,07 | 0,92 | 2,9 | 0,007 |
| Middle | 3,63 | 2,45 | 7,7 | 3,22 | 1,47 | 4,6 | ||
| Apical | 19,70 | 4,67 | 14,8 | 20,66 | 4,61 | 14,6 | ||
Note: Values are expressed in mm2.
| Third | Active Brackets | Passive Brackets | Sig. (p-value) |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Min. | Max. | Median | SE | SD | Min. | Max. | Median | SE | SD | ||
| Cervical | 0,00 | 7,80 | 1,34 | 0,77 | 2,45 | 0,00 | 5,82 | 2,25 | 0,78 | 2,48 | 0,333 |
| Middle | 0,01 | 5,05 | 0,86 | 0,51 | 1,60 | 0,00 | 5,51 | 0,99 | 0,53 | 1,67 | 0,285 |
| Apical | 0,00 | 11,81 | 6,28 | 1,46 | 4,63 | 0,05 | 12,34 | 6,61 | 1,39 | 4,40 | 0,575 |
| Total | 0,58 | 16,86 | 8,47 | 1,73 | 5,46 | 0,22 | 17,86 | 9,84 | 1,97 | 6,24 | 0,169 |
Note: Values are expressed in 10-3 mm3.
| Third | Active Brackets | Sig. (p-value) |
Passive Brackets | Sig. (p-value) |
||||
|---|---|---|---|---|---|---|---|---|
| Median | SE | SD | Median | SE | SD | |||
| Cervical | 1,34 | 0,77 | 2,45 | 0,010 | 2,25 | 0,78 | 2,48 | 0,007 |
| Middle | 0,86 | 0,51 | 1,60 | 0,99 | 0,53 | 1,67 | ||
| Apical | 6,28 | 1,46 | 4,63 | 6,61 | 1,39 | 4,40 | ||
Note: Values are expressed in 10-3 mm3.
| Third | Active Brackets | Passive Brackets | Sig. (p-value) |
||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Min. | Max. | Median | SE | SD | Min. | Max. | Median | SE | SD | ||
| Cervical | 46 | 1846 | 335 | 77 | 415 | 50 | 3157 | 519 | 153 | 751 | 0,480 |
| Middle | 49 | 1210 | 239 | 73 | 290 | 120 | 2546 | 508 | 141 | 615 | 0,005 |
| Apical | 68 | 2388 | 403 | 171 | 618 | 88 | 2611 | 481 | 203 | 705 | 0,611 |
| Total | 46 | 2388 | 324 | 57 | 437 | 50 | 3157 | 507 | 92 | 684 | 0,022 |
Note: Values are expressed in µm.
| Third | Active Brackets | Sig. (p-value) |
Passive Brackets | Sig. (p-value) |
||||
|---|---|---|---|---|---|---|---|---|
| Median | SE | SD | Median | SE | SD | |||
| Cervical | 334,8 | 77,1 | 415,4 | 0,354 | 518,7 | 153,4 | 751,3 | 0,403 |
| Middle | 239,3 | 72,6 | 290,3 | 508,0 | 141,1 | 615,0 | ||
| Apical | 403,2 | 171,4 | 617,8 | 480,6 | 203,5 | 704,9 | ||
Note: Values are expressed in µm.
A statistically significant difference was observed only in resorption depth within the middle root third, where the passive bracket group showed slightly greater resorption depth (p-value < 0.05).
In both groups, resorption extended beyond the cementum and involved the dentin.
In the active bracket group, 20% of resorption sites did not extend into the dentin, compared with 16% in the passive bracket group.
4. DISCUSSION
The present study evaluated early Orthodontically Induced Inflammatory Root Resorption (OIIRR) in maxillary first premolars subjected simultaneously to active and passive self-ligating brackets. Quantitative analysis demonstrated that both systems produced comparable levels of cementum and dentin resorption, with no significant differences in crater surface area, volume, or depth. These findings reinforce the growing evidence that bracket clip design alone does not substantially modify the early biological response of the periodontal ligament when comparable mechanical conditions are applied.
Consistent with our results, previous CBCT studies have reported no significant differences in OIIRR between self-ligating and conventional systems [21, 22]. More recently, Villaman-Santacruz et al. reported that variations in root resorption during dental movement were more strongly associated with the type of mechanical activation than with bracket design [23]. At the same time, the CBCT-based analysis of Lin et al. emphasized patient-specific biological factors as the main determinants of OIIRR risk [24]. Collectively, these findings align closely with the outcomes of the present investigation.
A major strength of this study lies in its intra-individual split-mouth randomized design, which inherently controls for inter-patient variability in root morphology, bone turnover, genetic susceptibility, and periodontal condition. This design enhances internal validity and allows a more accurate assessment of the mechanical differences between bracket systems. Regarding imaging methodology, conventional radiographs and CBCT studies [21, 22, 24, 25] often lack the spatial resolution required to detect shallow cementum-level defects. While scanning electron microscopy provides excellent surface detail [26, 27], it does not always allow for standardized volumetric quantification. In this study, high-resolution 3D confocal laser scanning microscopy was employed, offering three-dimensional accuracy comparable to modern micro-CT investigations [28-32] and enabling the reliable quantification of surface area, volume, and lesion depth.
In agreement with recent meta-analyses and clinical trials [16-18], although passive self-ligating brackets are designed for low-friction force delivery, the resulting biological response often remains equivalent to that of active systems. Our findings confirm the multifactorial nature of OIIRR, where factors such as force duration, individual molecular susceptibility, and complex hyalinization patterns play a more decisive role than the specific bracket clip design [1-3, 5]. The minor variations observed in the middle third of the root in our study likely reflect individual biological variability rather than a definitive mechanical disadvantage of either system.
From a clinical perspective, the fact that most resorption lacunae in both groups extended into the dentin is highly significant, as reparative potential at this depth is limited [25, 27]. This underscores the necessity for rigorous biomechanical control during the initial stages of alignment, irrespective of the bracket system used. Furthermore, contemporary evidence suggests that clinicians should implement personalized monitoring protocols, especially in patients identified with morphological or genetic risk factors [6-8, 24].
The study also offers methodological strengths, particularly the split-mouth randomized design, which effectively minimizes inter-patient biological variability, and the use of high-resolution confocal microscopy, which enhances the precision and reproducibility of quantitative measurements compared with conventional radiographic tools. However, certain limitations should be acknowledged. The sample size was constrained by strict inclusion criteria requiring bilateral premolar extractions, and the in vitro conditions do not replicate dynamic in vivo responses. Furthermore, the standardized observation period may not reflect long-term remodeling behavior. Larger clinical studies with extended follow-up intervals are warranted to validate and expand upon these findings.
In summary, active and passive self-ligating brackets produced comparable levels of early OIIRR, with no significant differences in the extent or severity of cementum–dentin involvement. These findings indicate that bracket clip design alone is unlikely to influence the risk of root resorption during the initial stages of orthodontic treatment, reinforcing the need for personalized biomechanical planning and diligent clinical monitoring. Importantly, throughout the nine-month treatment period, no major complications or serious adverse events were reported in either group. Specifically, no statistically significant differences were observed in the frequency of bracket debonding or in reported discomfort between the active and passive sides.
5. STUDY LIMITATIONS
While this study provides valuable quantitative insights into Orthodontically Induced Inflammatory Root Resorption (OIIRR) associated with self-ligating systems, certain limitations should be considered. The sample size was moderate and derived from a single institution, which may limit the extrapolation of results to broader populations. Nonetheless, the split-mouth design minimized inter-individual variability and strengthened internal validity. The use of an in vitro confocal microscopy model, although not replicating the full biological environment, allowed for highly precise and reproducible 3D evaluation of resorption craters. In addition, the observation period was intentionally standardized to control for the influence of treatment duration, though longer follow-up studies would further clarify cumulative biological effects. Future investigations, including larger and more diverse samples, as well as in vivo longitudinal analyses, are encouraged to expand upon the present findings.
CONCLUSION
The extent of orthodontically induced root resorption does not depend on the type of self-ligating bracket (active or passive). All extracted premolars exhibited resorption extending into the dentin, indicating irreversible cementum–dentin loss.
To minimize iatrogenic effects, orthodontic forces should always be maintained at the lowest biologically acceptable levels, consistent with tissue physiology and principles of tooth preservation.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| SD | = Standard Deviation |
| OIIRR | = Orthodontically Induced Inflammatory Root Resorption |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was granted by the Institutional Health Research Ethics Committee (CIEIS) of the School of Dentistry, National University of Córdoba, and authorization was obtained from the Council of Ethical Evaluation of Research in Health (CoEIS), Ministry of Health of Córdoba Province, Argentina (Approval Number: V.1.2011).
HUMAN AND ANIMAL RIGHTS
All procedures performed in this study involving human participants complied with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration.
CONSENT FOR PUBLICATION
All patients and their parents/guardians received both verbal and written explanations of the study and provided informed consent prior to participation.
AVAILABILITY OF DATA AND MATERIALS
The data of current study are available from corresponding author, [J.C.], on a reasonable request.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge the late Dr. AABP (†) for his valuable contribution to this study.

