All published articles of this journal are available on ScienceDirect.

Failure Patterns of Severely Compromised Endodontically Treated Anterior Teeth: A Comparative In Vitro Study of Two Restorative Approaches
Abstract
Introduction
This in vitro study aimed to compare the failure patterns of two restorative techniques in severely damaged, endodontically treated maxillary central incisors: (1) endocrowns fabricated from lithium disilicate ceramic (IPS e.max Press), and (2) quartz-fiber posts with composite resin cores and lithium disilicate crowns (IPS e.max Press).
Materials and Methods
Twenty freshly extracted human maxillary central incisors with intact roots, comparable in length, morphology, and size, were selected. The teeth were randomly allocated into two groups (n = 10): Group I, restored with lithium disilicate endocrowns (IPS e.max Press), and Group II, restored with quartz-fiber posts, composite resin cores, and lithium disilicate crowns (IPS e.max Press).
Specimens were mounted and tested using a universal testing machine. A compressive load was applied at a 45° angle to the middle third of the palatal surface at a crosshead speed of 0.5 mm/min until failure occurred. Failure patterns were recorded and analyzed using SPSS software (version 13).
Results
Statistical analysis revealed no significant differences in the distribution of failure patterns between the two groups (p > 0.05, 95% confidence level).
Discussion
This study compared endocrowns and post-and-core restorations for endodontically treated maxillary central incisors. Both techniques showed comparable fracture resistance, with failure modes differing mainly in location and repairability. Endocrowns demonstrated favorable outcomes due to their minimally invasive design and improved stress distribution. These findings support endocrowns as a conservative alternative while confirming that both approaches can provide clinically acceptable performance.
Conclusion
Within the limitations of this in vitro study, endocrowns fabricated from lithium disilicate (IPS e.max Press) exhibited failure patterns comparable to those of the conventional technique involving quartz-fiber posts, composite cores, and lithium disilicate crowns when restoring severely compromised endodontically treated anterior teeth.
1. INTRODUCTION
Endodontically treated anterior teeth represent a considerable restorative challenge, largely due to the substantial loss of tooth structure that occurs following pulp treatment. This structural reduction adversely affects the resistance form of the tooth and, if not adequately managed, may increase susceptibility to fracture [1]. Conventionally, retention in such cases has been achieved through the use of intra-radicular post-and-core systems [2]. Although these restorations have been associated with acceptable clinical performance, their placement often requires the removal of additional radicular dentin, reported in some cases to exceed 50% in maxillary incisors, which may further weaken the remaining tooth structure and increase the risk of catastrophic root fractures [3, 4].
The clinical performance of post-and-core restorations is influenced by several interrelated factors, most notably the amount of remaining coronal tooth structure, root canal anatomy, and the mechanical properties of the post material [5]. Various post systems are currently available, including metallic posts, fiber-reinforced posts (such as glass, quartz, and carbon fibers), as well as newer materials like zirconia and PEEK [6]. Recent studies suggest that selecting a post material with a modulus of elasticity closer to that of dentin may contribute to more favorable stress distribution within the root structure, potentially reducing the risk of catastrophic failure [7].
Although conventional guidelines advocate a post length equivalent to two-thirds of the root and a diameter not exceeding one-third of the root width, the actual biomechanical significance of these recommendations remains a subject of ongoing debate [8]. As a more conservative restorative approach, endocrowns were introduced to reduce the need for extensive radicular preparation. Early designs consisted of amalgam coronal–radicular cores with limited extension into the root canal system [9].
The contemporary concept of the endocrown was later defined by Bindl and Mörmann in 1999, who described it as a bonded ceramic restoration that derives its primary retention from the pulp chamber rather than from post placement, with little to no extension into the root canals [10]. Currently, endocrowns can be fabricated from a range of adhesive materials, including lithium disilicate, leucite-reinforced and feldspathic ceramics, as well as resin-based composite materials [10]. With the advancement of adhesive dentistry, endocrowns have gained wide clinical acceptance for posterior teeth, particularly in situations involving short roots, calcified canals, or reduced occlusal clearance [10].
Their reported advantages include conservative dentin preservation, procedural simplification, and decreased chairside time. Nevertheless, the application of endocrowns in anterior teeth remains relatively limited, primarily due to the lack of long-term clinical evidence and persistent clinician concerns regarding esthetics and biomechanics [11].
Accordingly, the present study aimed to assess the biomechanical performance of endocrowns compared with quartz fiber post–supported restorations in structurally compromised maxillary central incisors, to clarify the potential suitability of endocrowns for anterior applications.
1.1. Study Aim
The aim of this in vitro study was to evaluate and compare the failure patterns of lithium disilicate endocrowns used to restore severely compromised, endodontically treated maxillary central incisors with conventional lithium disilicate crowns supported by quartz fiber posts and composite resin cores.
2. MATERIALS AND METHODS
This study was approved by the Ethics Committee of the Faculty of Dentistry at Latakia University (approval No. 2379, dated 25-10-2021). It was conducted in accordance with the Declaration of Helsinki for human research [12].
2.1. Study Design
This study employed a randomized, controlled, and comparative in vitro experimental design.
Inclusion criteria: Recently extracted human maxillary central incisors with fully formed apices, single straight canals, no previous endodontic treatment, similar root dimensions (23 ± 1 mm), and intact roots free from cracks, caries, restorations, or resorption were included.
Exclusion criteria: Teeth with root caries, fractures, craze lines, internal or external resorption, calcified canals, curved roots, multiple canals, previous restorations, or structural anomalies were excluded from the study.
2.2. Sample Size Calculation
The required sample size was calculated using G*Power 3.1 software, assuming a 95% confidence level and a statistical power of 0.85. The study used a sample size of 20 specimens. Additionally, the tooth collection process was completed within 20 days.
2.3. Study Sample
The sample consisted of 20 recently extracted human maxillary central incisors obtained from patients who underwent extraction for periodontal reasons at the Faculty of Dentistry Clinics, Latakia University, Syria. Written informed consent was obtained from all patients for the use of extracted teeth for research purposes. All specimens were standardized in morphology and size (root length: 23 ± 1 mm; mesiodistal crown width: 7 ± 0.5 mm; buccolingual crown width: 9 ± 0.5 mm). After extraction, the teeth were thoroughly cleaned and stored in saline solution until testing. Once the sample was complete, the crown portion of each tooth was sectioned 2 mm above the Cemento-Enamel Junction (CEJ) using a straight handpiece and a 22-mm stainless steel laboratory separating disc [12].
All measurements and manual procedures, including preparation and cementation, were performed by a single operator (AK). Standardized root canal treatment was performed using a rotary endodontic system (Eighteeth E-Connect endo motor, Changzhou Sifary, China). Obturation was carried out with gutta-percha and an eugenol-free sealer. The specimens were then embedded in acrylic molds of uniform dimensions and randomly assigned to two equal groups (n = 10): Group I (Endocrowns), restored with lithium disilicate endocrowns (IPS e.max Press), numbered 1–10, and Group II (Post-and-Core Crowns), restored with quartz-fiber posts and composite resin cores, followed by lithium disilicate crowns (IPS e.max Press), numbered 11–20 [12].
2.4. Tooth Preparation
2.4.1. Group I (Endocrowns)
Excess gutta-percha at the entrance of the pulp chamber was removed carefully. The pulp chamber floor was prepared to a depth of 3 mm into the root canal while maintaining at least 1 mm of surrounding dentin. A 2-mm ferrule was established, along with a 1-mm circumferential finish line at the CEJ (Fig. 1).
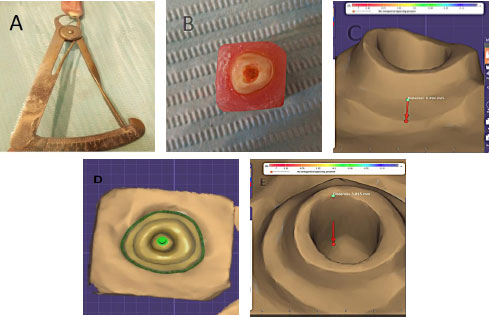
A) The remaining dentin thickness around the preparation in one of the abutments from group one. B) Occlusal view of the preparation in one of the abutments from group on. C) Display of the finish line in one of the abutments from group one after scanning with the milling scanner. D) Occlusal view after scanning. E) Measurement of the preparation depth inside the pulp canal after scanning.
2.4.2. Preparation of Group II Teeth
The specimens in this group were prepared to receive full-coverage lithium disilicate ceramic crowns (IPS e.max Press). Tooth preparation was performed under continuous water cooling using a round-ended tapered diamond bur (DiAMANT, Germany, 199X016 FG) to obtain a uniform 2-mm coronal ferrule and a 1-mm circumferential finish line at the cemento-enamel junction (CEJ). The diamond bur was replaced after every three preparations to maintain cutting efficiency. The finish-line width was verified using a calibrated periodontal probe [12].
A specific drill was used to prepare the post space to a depth of 8 mm inside the canal, corresponding to a post diameter of 1.4 mm, while maintaining 4–5 mm of apical gutta-percha. Subsequently, Quartz fiber posts (Quartz Fiber Resin Post, RTT, China) were cemented according to standard protocols. The canals were irrigated with 5.25% sodium hypochlorite (Canox, Syria), dried with oil-free air, and luted with a dual-cure self-adhesive resin cement (Breeze, Lot 8725242, Pentron, USA) following the manufacturer’s instructions. Cement was applied to the post, which was then placed inside the canal, and excess cement was removed using a microbrush. Light curing was performed from the buccal, palatal, and incisal aspects with an LED curing unit (Light Curing LED, Medical Hemao, China) at an intensity exceeding 1000 mW/cm2 for 60 seconds [12].
2.5. Composite Core Build-up
The coronal portion of each specimen was rebuilt using a composite resin core. Dentin was etched with 37% phosphoric acid (Eco-Etch, Ivoclar Vivadent, Liechtenstein) for 15 seconds, rinsed, and dried with oil-free air. A universal bonding agent (Tetric N-Bond Universal, Ivoclar Vivadent, Liechtenstein) was applied and light-cured for 15 seconds. The core was built incrementally using a nanohybrid composite (Tetric N-Ceram, Lot 23503, Ivoclar Vivadent, Liechtenstein), with each layer not exceeding 1.5–2 mm in thickness. Each increment was light-cured individually for 40 seconds using the same LED curing unit. After completing the core build-up (Fig. 2A), the preparation was refined using a round-ended tapered diamond bur to remove undercuts and ensure smooth continuity between the composite core and natural tooth structure (Fig. 2B and C) [12].
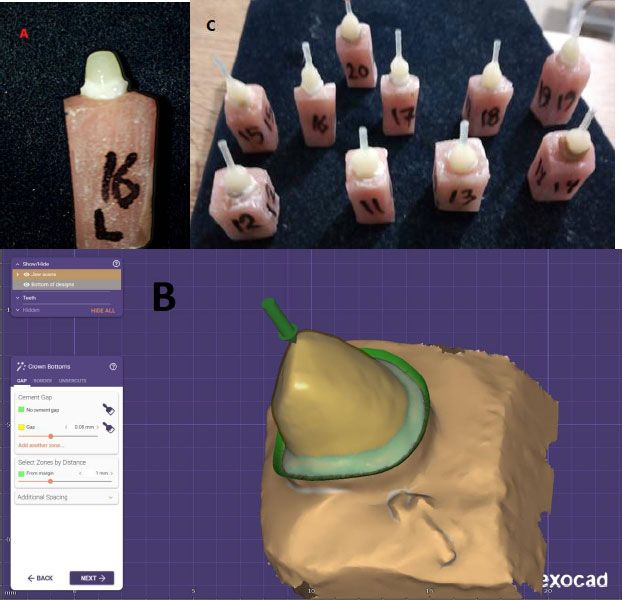
A) One of the abutments from group two. B) Occlusal view and measurement of the finish line width of one of the abutments from Group Two after scanning with the optical scanner. C) Specimens of Group II.
2.6. Standardized Tooth Dimensions in Group II (Fig. 3)
All prepared teeth in this group were standardized according to the following parameters: Ferrule height: 2 mm; finish line width: 1 mm; core height (from finish line to incisal edge): 7 mm; maximum mesiodistal core width: 7 mm; maximum buccolingual core width: 5 mm [12]; and impression and model fabrication.
After tooth preparation in both experimental groups, impressions were obtained using plastic stock trays and the double-mix, single-step technique with condensation silicone (Zetaplus Putty and Oranwash L Light Body, Zhermack, Italy). Casts were poured using type IV dental stone (Marmorock, Siladent, Germany) and transferred to the laboratory. All specimens were stored in saline for 3 days before laboratory procedures were performed [12].
Stone casts were scanned using a DGSHAPE scanner, and three-dimensional digital models were processed using CAD software (exocad DentalDB, version 2016). Standardized wax patterns were designed with the following dimensions (Fig. 3): Incisogingival height (from finish line): 10.5 mm; maximum mesiodistal width: 9.2 mm; and maximum buccolingual width: 7 mm.
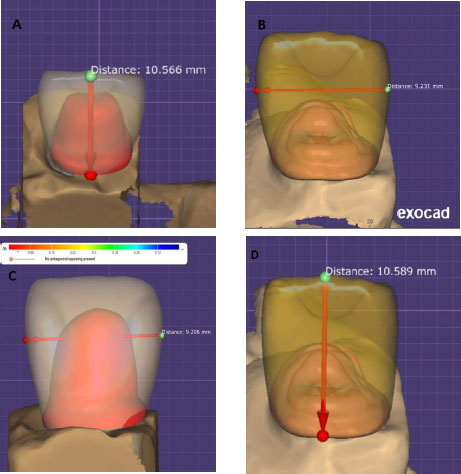
The measurements of the wax models before milling.
A 40-µm cement space was applied between the restoration and tooth walls. Wax discs (VeriCORE Mill Wax) were milled using a 5-axis dry milling unit (ROLAND® DGSHAPE DWX-52DCI) to produce standardized wax patterns with a 40-µm cement space. Margins were sealed with casting wax (Renfert), and 3-mm wax sprues (Renfert) were attached following the manufacturer’s recommendations (Fig. 4).
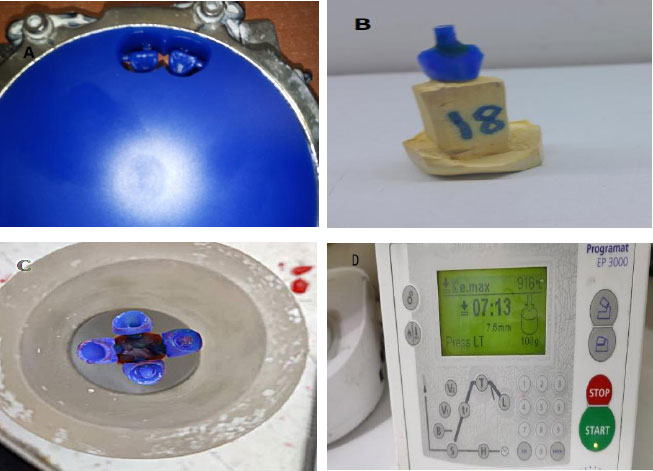
A) Wax disc milling. B) Wax model anchoring. C) Final waxing with pins on the injection crucible base. D) Setting up the thermal injection device.
2.7. Pressing and Finishing Procedures
The wax patterns were invested and processed using IPS Press Vest (Ivoclar Vivadent). Pressing was performed in a ceramic press furnace following the manufacturer’s protocol. The resulting restorations were conditioned with <1% hydrofluoric acid for 20 minutes, sandblasted with rubberized abrasive particles, rinsed, dried, and glazed according to the manufacturer’s instructions, producing restorations ready for cementation [12].
2.8. Cementation
The internal and marginal fit of each ceramic restoration was verified prior to cementation. Restorations were cleaned with alcohol, rinsed with water, and air-dried. The intaglio surface, including the intracanal extension, was etched with 9.5% hydrofluoric acid (Porcelain Etchant 9.5%, Lot 220005167, Bisco, USA) for 90 seconds, rinsed thoroughly for 1 minute, and air-dried. Two layers of silane coupling agent (Porcelain Primer, Lot 220004029, Bisco, USA) were applied and allowed to react for 1 minute [12].
On the tooth surface, preparations were cleaned with pumice powder and a brush, rinsed, and dried. Enamel and dentin were etched with 37% phosphoric acid (Lot T38390, Ivoclar Vivadent, Liechtenstein) for 15 seconds, rinsed thoroughly, and air-dried for 20 seconds. A universal bonding agent (Tetric N-Bond Universal, W08416, Ivoclar Vivadent, Liechtenstein) was then applied, gently air-thinned, and light-cured for 20 seconds [12].
A dual-cure resin cement (MetaCem, Meta Biomed, Germany) was mixed according to the manufacturer’s instructions and applied to the internal surface of each restoration. Restorations were seated with light finger pressure, and excess cement was removed. Light curing was performed on the buccal, lingual, mesial, and distal aspects for 40 seconds per surface using the same LED curing unit (Fig. 5).
A) Etching the internal surfaces of the restorations with 9.5% hydrofluoric acid. B) The chalky appearance of the porcelain after etching. C) Application of the dual bond agent (silane). D) Etching the abutments with 37% phosphoric acid. E) Applying bond. F) Application of the dual-cure resin cement. G) Curing the cement using a light-curing device.
All specimens were stored in physiological saline solution for 48 hours before mechanical testing (Fig. 6A-C). A comparison between the two groups is presented in Fig. (7).
(A and B) The final restoration after bonding. C) Applying oblique forces to the teeth at a 45-degree angle on a custom-made base.
Illustrates the final compound for both study groups.
2.9. Mechanical Testing
For fracture testing, each specimen was mounted in a custom-made base at a 45° angle to simulate functional loading. A knife-edge steel indenter (4-mm width) was positioned against the middle third of the palatal surface, and compressive loading was applied at a crosshead speed of 0.5 mm/min using a universal testing machine until failure occurred (Fig. 6C). Failure patterns were visually inspected (Fig. 7) and classified according to the categories used for the two experimental groups (Table 1). Statistical analysis was performed using SPSS software (version 13.1).
| Restorative Technique | Number of incisors | Percentage (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fracture of the restoration and tooth below the (CEJ). | Fracture of the restoration and tooth above the (CEJ). | Fracture of the Tooth below the (CEJ). | Fracture of the Restoration only. | Debonding of the Restoration. | Total | Fracture of the Restoration and Tooth below the (CEJ). | Fracture of the restoration and tooth above the (CEJ). | Fracture of the Tooth below the (CEJ). | Fracture of the Restoration only. | Debonding of the Restoration. | Total | |
| Endocrown restoration made of IPS e.max press extending 3 mm into the root canal | 3 | 3 | 1 | 3 | 0 | 10 | 30.0 | 30.0 | 10.0 | 30.0 | 0 | 100 |
| Quartz-fiber post with composite core and IPS e.max press crown | 2 | 0 | 0 | 7 | 1 | 10 | 20.0 | 0 | 0 | 70.0 | 10.0 | 100 |
| Total sample | 5 | 3 | 1 | 10 | 1 | 20 | 25.0 | 15.0 | 5.0 | 50.0 | 5.0 | 100 |
3. RESULTS
3.1. Sample Description
The study sample consisted of 20 extracted human maxillary central incisors with intact roots, standardized in length and morphology. The specimens were randomly divided into two equal groups (n = 10) according to the restorative technique, such as Group I consisting of lithium disilicate endocrowns (IPS e.max Press) extending 3 mm into the canal, and Group II comprising quartz-fiber posts and composite resin cores, followed by lithium disilicate crowns (IPS e.max Press).
3.2. Fracture Patterns
Fracture patterns were evaluated based on the visual assessment of each specimen after mechanical testing. The following patterns were identified: Fracture of the restoration and tooth below the CEJ (Fig 8A and B); fracture of the restoration and tooth above the CEJ (Fig. 8C and D); fracture of the tooth below the CEJ (Fig. 8E); fracture of the restoration only (Fig. 8F and G); and debonding of the restoration (Fig. 8H).
(A and B) Fracture of the restoration and tooth below the CEJ. (C and D) Fracture of the restoration and tooth above the CEJ. E) Fracture of the tooth below the CEJ. (F and G) Fracture of the restoration only. H) Debonding of the restoration.
Table 1 summarizes the distribution of fracture patterns according to the restorative technique.
3.3. Effect of Restorative Technique on Fracture Patterns
A Chi-square test was conducted to determine whether a statistically significant relationship existed between restorative technique and fracture pattern distribution, with Group I comprising lithium disilicate endocrowns (3-mm intracanal extension) and Group II consisting of quartz-fiber posts with composite resin cores and lithium disilicate crowns.
Table 2 presents the Chi-square analysis.
| The Studied variables = Fracture pattern × Restorative technique used | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Number of incisors (n) | Chi-square (χ²) | Degrees of freedom | p-value (Significance level) | Significance of differences | |||||
| 20 | 6.8 | 4 | 0.147 | No statistically significant differences | |||||
The p-value exceeded 0.05, indicating that no statistically significant differences were found between the two groups at the 95% confidence level regarding fracture pattern distribution.
3.4. Fracture Nature Assessment
Fractures were further classified as favorable or unfavorable based on their clinical reparability. The distribution of fracture types relative to restorative technique is illustrated in Fig. (9).
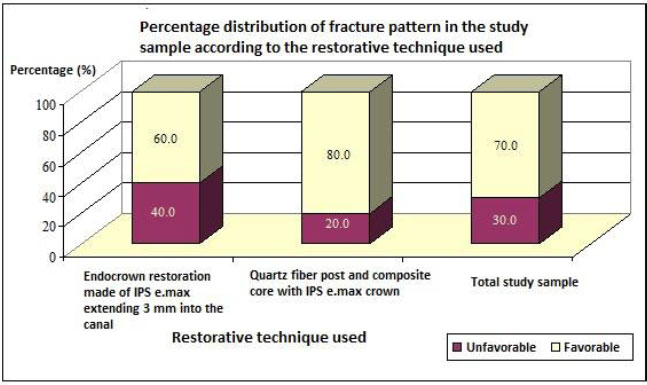
Percentage distribution of the results of the nature of fractures in the study sample according to the restorative technique used.
3.5. Effect of Restorative Technique on Fracture Nature
The effect of restorative technique on fracture type was evaluated using a Chi-square test to determine whether the choice of technique influenced the nature of fractures, with Group I consisting of lithium disilicate endocrowns (3-mm intracanal extension) and Group II comprising quartz-fiber posts with composite cores and lithium disilicate crowns.
Results are summarized in Table 3, presenting the statistical comparison of favorable and unfavorable fracture types between groups.
| The Studied variables = Nature of fracture × Restorative technique used | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Number of incisors | Chi-square value | Degrees of freedom | Significance level (p-value) | Significance of differences | |||||
| 20 | 6.8 | 4 | 0.147 | Not significant (NS) | |||||
3.6. Interpretation of Results
The obtained p-value was considerably greater than 0.05. This indicates that, at the 95% confidence level, there was no statistically significant difference in the distribution of fracture nature (favorable vs. unfavorable) between the two restorative approaches: lithium disilicate endocrowns (IPS e.max Press) with a 3 mm intracanal extension and quartz fiber–reinforced resin posts with composite cores and lithium disilicate crowns (IPS e.max Press).
4. DISCUSSION
This study evaluated two restorative approaches for structurally compromised, endodontically treated maxillary central incisors: (1) endocrowns fabricated from IPS e.max ceramic with a 3 mm intracanal extension, and (2) quartz fiber–reinforced resin posts with composite cores and IPS e.max crowns. The specimens were carefully selected to ensure similarity in morphology and dimensions, which resemble the clinical biomechanical conditions. The specimens were stored in saline for 20 days before testing, thus not affecting mechanical properties such as hardness [13].
Maxillary central incisors were chosen for their significant esthetic and functional importance. In addition, there is a limited number of studies evaluating endocrown restorations in anterior teeth [7]. Traditional post-and-core techniques often require the removal of significant amounts of sound tooth structure and may be a challenge during endodontic retreatment, especially in single-rooted teeth, in which post removal increases the risk of root fracture [14]. Furthermore, teeth with limited vertical dimension may prevent the usage of conventional posts and crowns [15], supporting the investigation of endocrowns as a more conservative restorative alternative.
Endocrowns are widely recognized for their minimally invasive design, reduced chairside time, and favorable esthetic outcomes. In addition, they provide a stable coronal seal that may limit bacterial microleakage, leading to improve the long-term prognosis of endodontically treated teeth. Another advantage of endocrowns is that retreatment is generally less complex compared with conventional post-and-core systems. Furthermore, several studies have reported that endocrowns show higher stability and fracture resistance, along with reducing the catastrophic root fractures [16].
A 3 mm intracanal extension was selected for the endocrown group, aligned with previous findings suggesting no significant differences in fracture resistance between 3 mm and 6 mm extensions in IPS e.max endowcrowns [17]. In the post-and-core group, canal preparation extended to two-thirds of the root length (approximately 8 mm) [18], following established recommendations. IPS e.max was chosen due to its excellent mechanical properties and esthetic advantages [19], and composite core dimensions adhered strictly to the manufacturer’s guidelines.
A standardized 1-mm finish line was prepared on both groups to ensure uniform stress distribution. CAD/CAM technology was used for designing and milling the wax patterns to ensure the accuracy of restoration fabrication [20].
The teeth were embedded in acrylic resin blocks to simulate clinical circumstances with a modulus of elasticity similar to that of natural bone [21]. Periodontal ligament simulation was ignored, aligning with studies showing its limited influence on fracture resistance outcomes [21].
The results revealed no statistically significant differences in the distribution of failure modes between the two restorative approaches. In the post-and-core group, failure was most frequently limited to the restoration itself, which can be attributed to the elastic modulus of quartz fiber posts (45–49 GPa) being closer to dentin (14–18 GPa) [22]. This biomechanical compatibility allows the post to flex under load, reducing stress concentration in the root and lowering the risk of catastrophic fractures. These observations are consistent with Sebastià et al. [23] and Zhou and Wang (2013) [24]. Stress distribution along the root in fiber post restorations explains why coronal restorative fractures predominated in this group [25].
Conversely, failure modes in the endocrown group were more heterogeneous, with one case of tooth fracture below the Cemento-Enamel Junction (CEJ). This could be explained by the strong micromechanical bonding of lithium disilicate ceramics with dental tissues, along with the reduced number of adhesive interfaces. Furthermore, the absence of an intraradicular post transfers functional stresses coronally, thereby localizing most failures at the restoration level rather than within the root.
Failure modes were categorized as favorable (restoration fracture, debonding, or fracture above the CEJ) or unfavorable (fracture below the CEJ). Favorable failure patterns occurred in 80% of group I specimens and 60% of group II specimens, although the difference was not statistically significant. Interestingly, repairable failures appeared more frequently in the post-and-core group. This may be due to the monoblock-like integration of the endocrown with the tooth structure and the involvement of the root in intracanal fractures associated with the 3 mm extension.
These findings are consistent with the outcomes of Al Fodeh et al. (2023) [26] and Guo et al. (2016) [27], both of which reported no significant differences in the frequency of favorable failure modes between endocrowns and fiber-post–supported ceramic crowns. Our results also align with those of Bankoğlu Güngör et al. (2017) [28], who reported that lithium disilicate endocrowns more often led to tooth fractures, whereas fiber-post restorations tended to fail at the restoration level. However, their study did not classify failure modes as favorable or unfavorable. Also, Chang et al. (2009) [29] found no significant differences between endocrowns and glass fiber post-supported crowns, noticing that unfavorable failures predominated in both groups. This discrepancy may be attributed to methodological differences, including the use of leucite-reinforced ceramics, CEREC CAD/CAM systems, and axial loading protocols.
In contrast, our results differ from those reported by Pedrollo et al. (2017) [30], who observed no favorable failure patterns in the endocrown group, whereas 37.5% favorable failures were recorded in the fiber-post group. This discrepancy may be attributed to differences in study design. In their investigation, endocrowns featured a 5 mm intracanal extension, which could have adversely affected root integrity, and no cervical ferrule was prepared in the post-and-core group. Conversely, our protocol included a 2 mm ferrule, a design feature known to improve fracture resistance and decrease the unfavorable root fractures [31]. Additionally, methodological variations, such as their use of mandibular premolars and the application of 1,200,000 cyclic loading cycles prior to fracture testing, may have further contributed to the observed differences in outcomes.
Moving beyond the descriptive comparison of failure patterns, it is important to consider the biomechanical factors that may explain how the two restorative systems respond to oblique loading. In the endocrown group, retention is achieved through a single, continuous adhesive interface between the lithium disilicate restoration and the prepared cavity walls. This simplified bonding configuration limits the number of potential weak interfaces and may improve stress distribution. In addition, micromechanical retention is enhanced by hydrofluoric acid etching and silane application, which contribute to a more stable adhesive bond.
Previous studies have demonstrated that etched lithium disilicate forms a durable hybrid layer with resin cement. This strong bond improves the cohesive integrity of the tooth–restoration complex [32, 33]. As a result, failures in endocrowns tend to occur within the ceramic or the underlying tooth structure rather than at the adhesive interface. This pattern is consistent with the mixed failure modes observed in the present study.
However, this strong adhesion also has biomechanical consequences. Because lithium disilicate has a high elastic modulus (~95 GPa), stresses generated under oblique loading tend to concentrate at the cervical margins and along the internal walls of the pulp chamber. Finite element analyses have shown that endocrowns can promote tensile stress accumulation in the cervical dentin. This effect is mainly related to the rigidity of the ceramic and its limited ability to absorb deformation, especially when intracanal extensions are present [34, 35].
In contrast, the post-and-core system incorporates multiple adhesive interfaces (dentin–cement, cement–fiber post, composite core–tooth, core–crown), each of which can act as a potential stress-attenuating interface. The quartz fiber post, with an elastic modulus closer to that of dentin (≈45–50 GPa), promotes more favorable stress distribution along the root. This elastic compatibility reduces stress concentration in apical and cervical regions and redirects deformation coronally, making restoration-level fractures more common and root-level fractures less frequent [36, 37]. Additionally, the composite resin core acts as a stress-dissipating layer, limiting crack propagation toward the radicular dentin and supporting the prevalence of repairable coronal fractures [38].
Several investigations have shown that endocrowns tend to concentrate higher stresses in the cervical dentin. In contrast, fiber-post restorations demonstrate a more uniform stress distribution, largely due to the similarity between the elastic modulus of the post and that of natural dentin [35, 39]. These biomechanical differences may help explain the distinct failure tendencies observed between the two groups, even though no statistically significant difference in overall failure pattern distribution was detected in the present study.
5. STUDY LIMITATIONS
This in vitro study may not fully replicate the complexities of the oral environment, including variable loading patterns and thermal fluctuations. The relatively small sample size may limit the generalizability of the findings. Additionally, periodontal ligament simulation and long-term fatigue loading were not performed, which may have influenced the clinical relevance and applicability of the results.
CONCLUSION
No statistically significant differences were observed in the failure patterns between lithium disilicate endocrowns and quartz fiber post–composite core–supported lithium disilicate crowns used to restore structurally compromised, endodontically treated anterior teeth.
Within the limitations of this in vitro study, both restorative techniques demonstrated comparable mechanical performance.
The endocrown design may represent a more conservative restorative alternative; however, its clinical applicability warrants further investigation.
Future long-term clinical and laboratory studies incorporating fatigue loading and thermocycling protocols are recommended to better simulate intraoral conditions.
AUTHORS’ CONTRIBUTIONS
The authors confirm contribution to the paper as follows: A.K., R.S.: Study conception and design; A.K., R.S.: Data collection; A.K., R.S.: Analysis and interpretation of results; A.K., R.S., Z.A.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| CEJ | = Cemento-Enamel Junction |
| CAD/CAM | = Computer-Aided Design / Computer-Aided Manufacturing |
| IPS e.max Press | = Ivoclar Pressed Lithium Disilicate Ceramic |
| PEEK | = Polyetheretherketone |
| SPSS | = Statistical Package for the Social Sciences |
| LED | = Light Emitting Diode |
| HF | = Hydrofluoric Acid |
| NaOCl | = Sodium Hypochlorite |
| Gpa | = Gigapascal |
| mm | = Millimeter |
| µm | = Micrometer |
| Mpa | = Megapascal |
| p-value | = Probability value |
| SD | = Standard Deviation |
| CI | = Confidence Interval |
| CEREC | = Chairside Economical Restoration of Esthetic Ceramics |
| E.max | = Lithium Disilicate Ceramic System |
| N | = Newton |
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This study was approved by the Ethics Committee of the Faculty of Dentistry at Latakia University, Syrian Arab Republic (approval No. 2379, dated 25-10-2021).
HUMAN AND ANIMAL RIGHTS
All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or research committee and with the 1975 Declaration of Helsinki, as revised in 2013.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
Declared none.

