All published articles of this journal are available on ScienceDirect.

The Influence of Different Dental Implant Abutment Materials on the Color of Lithium Disilicate Crowns: A Combined In Vitro and Clinical Study
Abstract
Introduction
Dental implants in the anterior region represent a reliable and esthetically pleasing alternative to traditional bridges. Titanium abutments are considered the gold standard in implant dentistry; however, their use in esthetic zones often results in gray discoloration, particularly when combined with all-ceramic restorations or in patients with thin peri-implant tissues. Zirconia abutments have been proposed as an alternative to overcome these limitations. This study aimed to evaluate the effect of different abutment materials on the color change of lithium disilicate crowns through both in vitro and clinical assessment.
Materials and Methods
Thirty lithium disilicate crowns (IPS e.max CAD) of standardized central incisor form were fabricated and distributed equally among three groups: (1) titanium abutments, (2) zirconia abutments with a titanium base, and (3) titanium abutments coated with opaque material. Crowns were placed on the respective abutments with glycerin as an intermediate medium, and color change was measured using the Easy Shade device. Data were analyzed with the Kruskal-Wallis test due to non-normal distribution.
Results
Significant differences were observed among the groups. Lithium disilicate crowns supported by titanium abutments demonstrated clinically unacceptable color changes (ΔE = 9.7). Zirconia abutments with a titanium base produced color changes closely resembling natural dentition (ΔE = 6.1), while opaque-coated titanium abutments yielded clinically acceptable results (ΔE = 7.8).
Discussion
The results indicate that the abutment material significantly influences the final color of lithium disilicate crowns. Zirconia abutments effectively mask the underlying metallic hue due to their high radiopacity and light-scattering properties, while opaque coating provides a viable and more affordable alternative to mitigate the graying effect of titanium abutments.
Conclusion
Within the study limitations, zirconia abutments with titanium bases and opaque-coated titanium abutments are recommended over conventional titanium abutments in the anterior region to achieve superior esthetic outcomes with lithium disilicate crowns.
Clinical Trial Registration Number
This study is registered with the Research Registry under the identifying number: researchregistry11472, and the reference hyperlink is: https://www.researchregistry.com/browse- the-registry#home/
1. INTRODUCTION
Dental implants have become a widely adopted solution for the replacement of missing teeth, with success rates reaching up to 97% within the first ten years and 75% over the following decade [1]. One of the main components of a dental implant is the abutment, which serves as the intermediate structure between the implant and the crown, providing stability and support for the prosthesis [2]. Commonly used abutment materials include titanium, cobalt-chromium, zirconia, and gold [3].
In recent years, polyetheretherketone (PEEK) has gained significant attention as a promising alternative to conventional titanium (Ti) in the fabrication of implant abutments. Unlike titanium, PEEK exhibits favorable esthetic properties due to its tooth-like color and translucency, which help prevent dark shading of peri-implant soft tissues, which is a common concern in the anterior aesthetic zone. Moreover, PEEK demonstrates excellent biocompatibility, with a lower risk of allergic reactions compared to metal alloys, making it suitable for patients with hypersensitivity concerns [4, 5]. Recent studies have also highlighted the biomechanical advantages of PEEK abutments, including a modulus of elasticity closer to that of natural bone, which may help reduce stress shielding and improve load distribution at the implant–bone interface [6, 7]. Furthermore, advancements in digital dentistry have facilitated the precise CAD/CAM fabrication of custom PEEK abutments, enhancing both clinical efficiency and prosthetic fit [8, 9]. The ongoing development of PEEK-based composites, such as carbon fiber-reinforced PEEK, continues to expand its potential as a durable and clinically reliable abutment material for long-term provisional and definitive restorations.
Titanium and cobalt-chromium abutments are known for their high strength; however, they may cause grayish discoloration beneath lithium disilicate crowns or the peri-implant mucosa, which compromises esthetics. To overcome this issue, zirconia abutments were developed, offering color compatibility closer to natural teeth [10]. Nevertheless, monolithic zirconia abutments are susceptible to fracture at the implant–abutment connection, particularly in scenarios of off-axis loading or in small-diameter implants [11]. This brittleness is a concern for long-term reliability. To overcome this limitation while preserving esthetics, two-piece hybrid abutments were developed, consisting of a zirconia superstructure cemented or bonded onto a titanium base. This design leverages the superior fatigue resistance and ductility of titanium at the critical connection interface while utilizing zirconia for its optimal soft-tissue response and color properties in the supragingival region [12].
Titanium bases provide optimal strength, biocompatibility, and compatibility with CAD/CAM technology, allowing efficiency in fabrication [13]. A key advantage of titanium bases is their retrievability: the crown and abutment can be removed together, similar to custom abutments or screw-retained systems. Additionally, crowns may be bonded to the abutment extraorally, reducing the risk of peri-implant inflammation from excess cement, after which the abutment is screw-retained into the implant [14].
Because of zirconia’s esthetics, fracture resistance, and biocompatibility, it has been widely used in implant abutments [15]. CAD/CAM-fabricated zirconia abutments are among the most widely applied technologies worldwide, particularly for anterior esthetic restorations [16]. Zirconia abutments may be fabricated with or without a metallic base; however, studies have shown that incorporating a titanium base enhances the fracture resistance of zirconia abutments due to zirconia’s inherent brittleness [17].
Zirconia demonstrates mechanical properties comparable to stainless steel, with tensile strength ranging between 900–1200 MPa, compressive strength up to 2000 MPa, and flexural strength up to 1132 MPa, in addition to excellent biocompatibility and high esthetics [18]. Studies have confirmed high survival rates of ceramic crowns supported by zirconia abutments on implants [19]. Research has also indicated that tetragonal zirconia implants exhibit superior physical properties compared to titanium implants [1].
Most zirconia implants have been produced as one-piece designs. However, this design presents significant limitations: the surgical phase becomes more demanding to ensure alignment between implant placement and the final prosthesis, angulated abutments are unavailable, and the implants are directly exposed to functional forces from the tongue or mastication. Furthermore, there are no long-term clinical studies on this type of implant, and reported failure rates are higher compared to two-piece titanium implant systems, largely due to screw-retention challenges [20].
Restoring missing anterior teeth with prostheses that meet high biological, mechanical, and esthetic demands is of utmost importance [21]. For this reason, alternatives to titanium abutments have been sought to address grayish discoloration of peri-implant mucosa or beneath all-ceramic crowns. Zirconia has emerged as the preferred material due to its superior mechanical properties compared to other ceramics [12]. Current zirconia abutment options include prefabricated types or CAD/CAM-customized abutments connected to the implant via a titanium base. Mechanically, there is no significant difference between prefabricated and CAD/CAM abutments, although CAD/CAM abutments offer greater customization and angulation [22].
Studies have demonstrated that zirconia abutments with titanium bases are stronger than full-zirconia abutments [16]. A conical design of the zirconia cap on a titanium base with a semi-shoulder configuration has been shown to provide the most stable interlocking between components [23].
It is important to note that luting cements used for conventional tooth-supported fixed restorations do not necessarily exhibit the same behavior in implant-supported restorations [24]. For example, zinc oxide eugenol cement, commonly used as a temporary luting agent on natural abutments, may function as a temporary or semi-permanent cement for implant-supported crowns [25]. Temporary cements are characterized by high solubility and low tensile strength, which may be advantageous in implant restorations by facilitating retrievability in cases such as peri-implantitis. Examples include zinc oxide eugenol and zinc oxide non-eugenol cements [26]. However, prosthesis decementation rates have been reported as high as 17.6% with temporary cements [27].
Semi-permanent cements, such as zinc phosphate and glass ionomer, provide adequate retention while reducing the risk of frequent debonding [28]. Both also allow retrievability when necessary [29]. Studies have shown high retention rates and negligible decementation with these cements in implant restorations [30].
In certain cases, clinicians may prefer permanent cementation of implant-supported restorations. Permanent cements must possess properties that prevent future complications affecting peri-implant tissues or the restoration itself. Resin cements and resin-modified glass ionomer cements are the most commonly used permanent agents [31]. However, resin cements contain tertiary amines, which have been associated with color instability [32]. To mitigate excess cement complications, extraoral bonding of perforated crowns to the abutment, followed by screw-retained fixation, has been advocated as a successful method [33].
The quantification of color change is central to evaluating esthetic outcomes and is typically measured using the CIELAB color system and expressed as ΔE (Delta E). The clinical relevance of ΔE values is interpreted through perceptibility and acceptability thresholds. A color change with a ΔE value < 1 is generally considered imperceptible to the human eye. Values between 1.0 and 3.5 are perceptible but may be clinically acceptable, whereas a ΔE > 3.5 is typically considered visually unacceptable. It is important to note that these thresholds can be influenced by the duration of observation and surrounding environmental conditions; however, a change exceeding the 3.5 threshold is immediately noticeable in a clinical setting and often leads to patient dissatisfaction [34].
Furthermore, the duration of exposure to the restoration can affect the observer's ability to detect color differences. Short-term observations during a clinical visit may mask subtle color mismatches that become more apparent over time, especially under varying lighting conditions or as the patient adapts to the prosthesis. Therefore, while immediate ΔE measurements provide valuable initial data, long-term follow-up is essential to fully assess the aesthetic stability and patient acceptance of implant-supported restorations.
This study aims to evaluate the color change of lithium disilicate crowns placed on different implant abutments and to identify the optimal abutment–crown combination to achieve the best esthetic outcome in anterior restorations.
2. MATERIALS AND METHODS
To address the research purpose, the investigators designed and implemented a study comprising both in vitro and clinical components. The study was conducted in the Department of Fixed Prosthodontics, Faculty of Dentistry, Tishreen University, between 2019 and 2022 in accordance with the Declaration of Helsinki. Ethical approval was obtained from Tishreen University (Approval No. 486, Session 8, February 4th, 2019).
2.1. In Vitro Sample
A statistical power analysis using the G*Power program indicated that the required sample size was 10 crowns per tested variable, totaling 30 lithium disilicate crowns. The error value was 0.05, the effect size adopted for this type of study was 0.5, and the statistical power was 0.17, which is close to the reference value of 0.2 commonly used in such tests.
Ten crowns were allocated to each abutment type. Table 1 provides a description of the in vitro sample, and Fig. 1 illustrates the distribution of study groups according to abutment type.
| Study Group | Number Of Crowns | Percentage |
|---|---|---|
| Zirconia abutments (de zer) | 10 | 33.3% |
| Titanium abutments (de metal) | 10 | 33.3% |
| Opaque-coated titanium abutments (de opa) | 10 | 33.3% |
| Total | 30 | 100% |
Distribution of study groups by abutment type.
The in vitro sample consisted of 30 lithium disilicate crowns (IPS e.max CAD), numbered 1–30, designed as standardized central incisors with the following dimensions: 8 mm length, 6 mm width at the contact points, 5 mm width at the cervical region, 1.37 mm thickness at the incisal and middle thirds, and 0.7 mm thickness at the cervical third.
Additionally, 30 titanium base abutments (Bio3, Germany) were used. Ten zirconia copings with a thickness of 0.30 mm were fabricated to fit over the titanium bases.
2.1.1. Materials and Devices for the In Vitro Study
Materials:
- 30 lithium disilicate crowns (IPS e.max CAD, shade A1).
- IPS e.max CAD discs (shade A1, Roseta).
- 30 titanium bases (Bio3, Germany).
- 30 implant analogs (Bio3).
- 10 zirconia copings (shade A1, Semphony) for titanium bases.
- Opaque material (shade A1, Initial, Germany).
- Pure glycerin.
Devices:
- Easy Shade (VITA, Germany) for shade measurement.
- CAD/CAM milling unit (ARUM Dental) for crown fabrication.
2.1.2. Experimental Groups and Procedure
- Group 1 (de metal): 10 lithium disilicate crowns and 10 titanium abutments. Abutments were fixed onto implant analogs in a gypsum model, crowns were seated with pure glycerin, and after 24 hours, color change values were recorded using the Easy Shade device (Fig. 2).
- Group 2 (de zer): 10 lithium disilicate crowns and 10 zirconia abutments (titanium base + zirconia coping). Abutments were assembled without bonding, crowns were placed with pure glycerin, and color measurements were taken after 24 hours (Fig. 3).
- Group 3 (de opq): 10 lithium disilicate crowns and 10 titanium abutments coated with opaque. Crowns were seated on the opaque-coated abutments with glycerin, and color measurements were taken after 24 hours (Fig. 4).
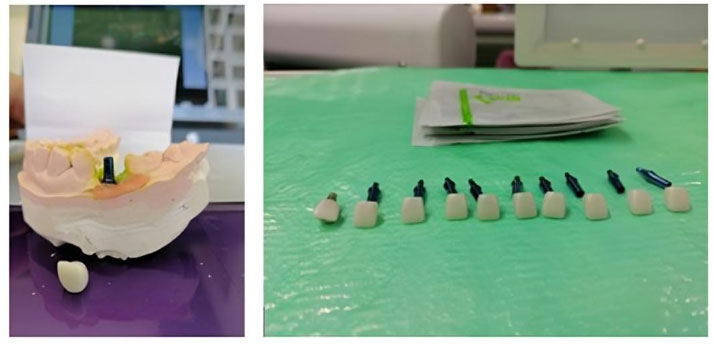
Titanium abutments.
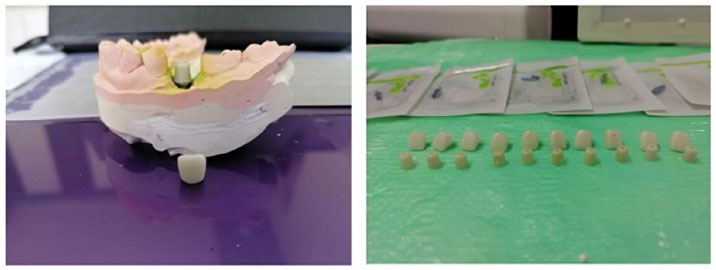
Zirconia abutments.
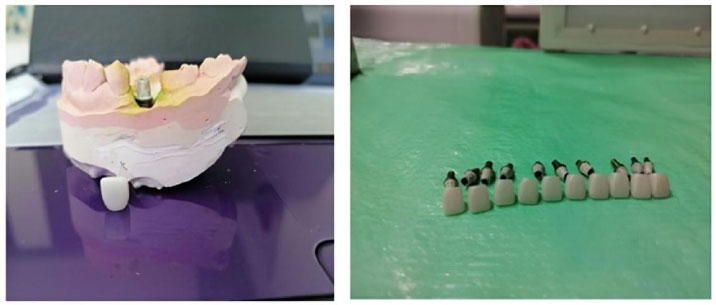
Lithium disilicate crowns with titanium abutments coated with opaque.
2.1.3. Easy Shade Protocol
1. Calibrate the device.
2. Activate the device.
3. Select “Check restoration shade.”
4. Select crown shade (A1 in this study).
5. Record color change (ΔE) (Fig. 5).

Easy shade protocol.
2.2. Clinical Study
2.2.1. Clinical Sample
The clinical sample included 8 titanium implants (Bio3), distributed among 4 patients aged 20–55 years (Fig. 6) Table 2 shows patient distribution by gender.
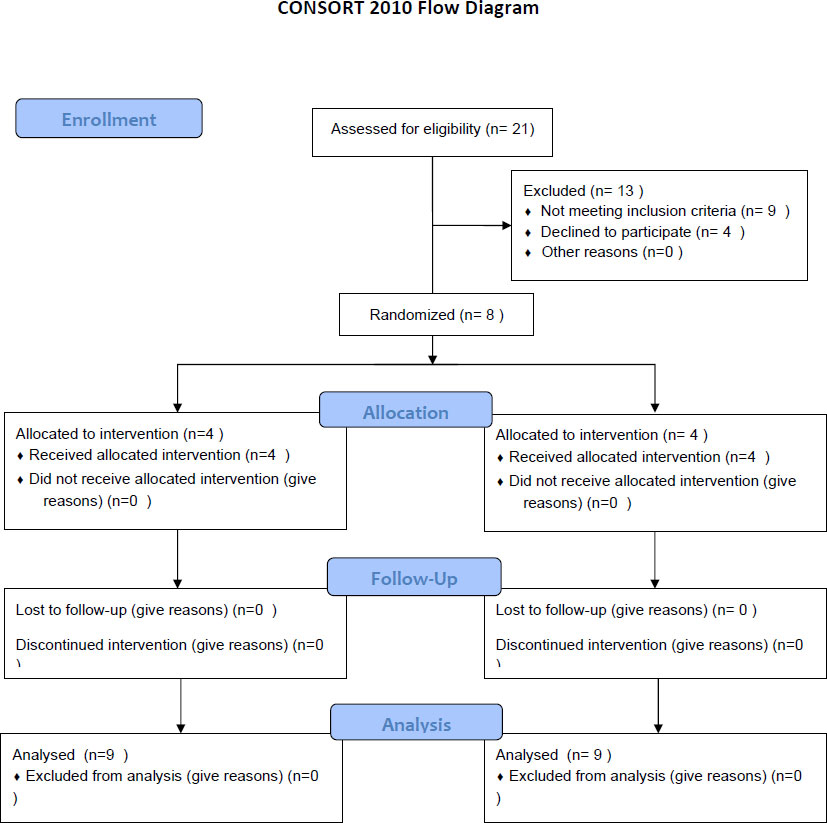
Consort flow diagram.
| Gender | Number of Patients | Percentage |
|---|---|---|
| Male | 2 | 50% |
| Female | 2 | 50% |
A total of 16 lithium disilicate crowns were placed on the implants, equally divided between zirconia abutments and opaque-coated titanium abutments (Table 3).
| Study Group | Number of Crowns | Percentage |
|---|---|---|
| Zirconia abutments | 8 | 50% |
| Opaque-coated titanium abutments | 8 | 50% |
| Total | 16 | 100% |
2.2.1.1. Inclusion Criteria
- Patient age between 20–55 years.
- No systemic diseases contraindicate implant surgery (cardiac, endocrine, hematologic, immunologic, or acute infections).
- Suitable local indication for implant placement (loss of maxillary central incisors adjacent or contralateral).
- Patient consent and commitment to follow-up.
2.3. Patient Acceptance Protocol and Surgical Planning
The surgical procedures for implant placement were performed according to standardized protocols, and all surgeries were performed at the Faculty of Dentistry, Tishreen University.
After confirming patient eligibility according to the study’s inclusion and exclusion criteria, written informed consent was obtained, and each patient signed an authorization form.
1. Radiographs were obtained to assess bone condition at the intended implant site.
2. Surgical planning was conducted using CBCT imaging to evaluate bone density and determine the expected implant position.
3. A clinical examination was performed, and based on both clinical and radiographic findings, a case-specific form was completed for each patient. This assessment included general health status, the local condition of the implant site, and the suitability of the occlusal and prosthetic relationships.
4. A total of 8 implants were placed in the patients’ jaws.
5. A two-stage surgical protocol was employed for implant placement.
2.4. Surgical Procedure Planning
The surgical procedures were planned and carried out as follows:
1. Patients were anesthetized locally using the appropriate anesthetic technique for each case.
2. A crestal incision was made at the edentulous ridge, with mesial and distal releasing incisions to elevate the flap.
3. A full-thickness mucoperiosteal flap was raised at the implant site.
4. Using the manufacturer-supplied implant motor and the sequential drills provided in the surgical kit, osteotomies were prepared to the diameter of each planned implant.
5. The implant fixtures were inserted in their positions with the appropriate torque (Figs. 7 and 8).
6. Suturing was performed according to the specific needs of each case.

Implant insertion.

Panoramic view for implant insertion.
2.5. Final Prosthetic Protocol
1. Gingival formers were placed for 7–10 days (Fig. 9).
2. Transfer copings were placed, and impressions were taken using the open-tray technique.
3. Impressions were poured and sent to the dental laboratory.
4. Zirconia abutments were cemented to titanium bases using glass ionomer cement.
5. Titanium bases were opaqued in the laboratory using an opaquer.
6. Abutments were fixed onto the implants (Fig. 10).
7. Lithium disilicate crowns were then cemented onto the abutments using a dual-cure resin cement (Fig. 11).

Healing cap insertion.

Zirconia abutment at the site of tooth #10, Opaque titanium abutment (with opaquer) at the site of tooth #7.
Final restoration.
2.6. Clinical Study Methodology
The clinical procedures were carried out as follows:
1. The color change value (∆E) was measured for lithium disilicate crowns cemented on two types of abutments, distributed as follows:
° 16 crowns, all shade A1.
° 16 abutments: 8 zirconia abutments with titanium bases and 8 titanium bases opaqued with opaquer material.
The crowns and abutments were repeatedly removed and reattached to the 8 implants, and measurements were taken using the Easy Shade device.
2. Patient satisfaction with the esthetic appearance of both abutment types was assessed.
2.7. Statistical Methods
To achieve the study objectives, Excel software and G*Power were used for data analysis.
- A significance level of 5% (p-value < 0.05), corresponding to a 95% confidence interval, was adopted to interpret the results.
- The following statistical tests and measures were applied:
- Means, standard deviations, variance, maximum, and minimum values.
- LSD test.
- Normality testing using the Kolmogorov–Smirnov (K-S) test.
3. RESULTS
3.1. Laboratory Results
3.1.1. Laboratory Findings
Table 4 presents the color difference values (ΔE) of the first group (lithium disilicate crowns on titanium abutments), the second group (lithium disilicate crowns on zirconia abutments), and the third group (lithium disilicate crowns on opaqued titanium abutments).
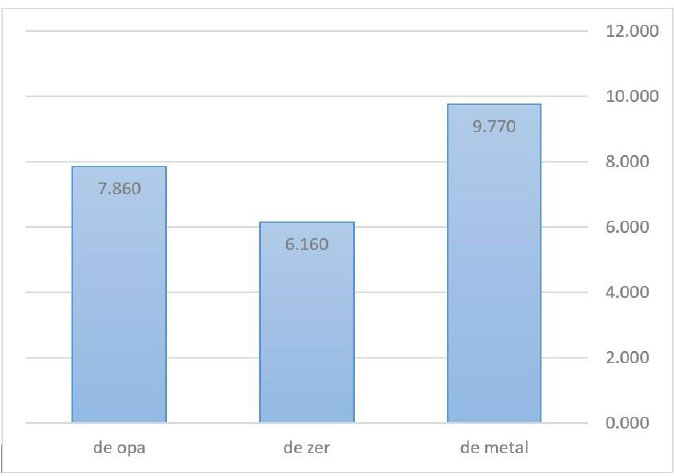
Using the Easy Shade device, the mean ∆E values (Fig. 12) for each group were:
| Group 1 | Crown | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| ΔE | 9.8 | 9.7 | 9.6 | 9.8 | 9.7 | 9.9 | 9.8 | 9.7 | 9.8 | 9.9 | |
| Group 2 | Crown | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| ΔE | 6.3 | 5.8 | 6.4 | 6.0 | 6.3 | 6.1 | 6.3 | 6.2 | 6.3 | 5.9 | |
| Group 3 | Crown | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
| ΔE | 8.1 | 8.0 | 8.1 | 7.8 | 8.0 | 7.9 | 7.7 | 7.8 | 7.8 | 7.4 |
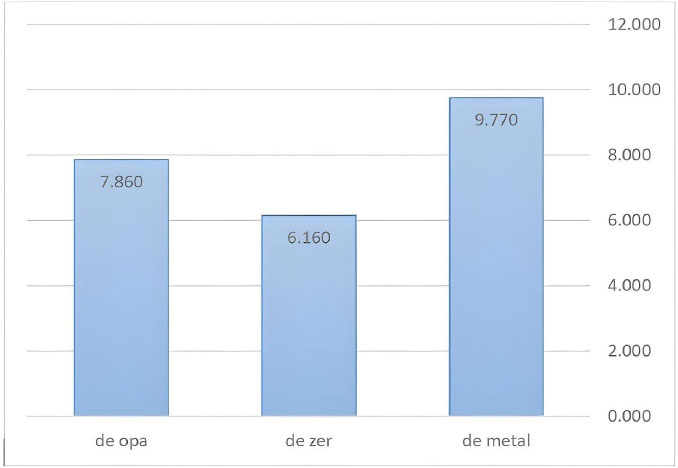
Comparison between the mean values in the three groups.
- Group 1 (Ti abutments): ∆E = 9.7
- Group 2 (Zr abutments): ∆E = 6.1
- Group 3 (Opaqued Ti abutments): ∆E = 7.8 (Table 5)
The difference between Group 1 and Group 2 was 3.6, and between Group 1 and Group 3 was 1.9.
| Group | N | Mean | Std | Min | Max |
|---|---|---|---|---|---|
| Ti (de metal) | 10 | 9.770 | 0.095 | 9.60 | 9.90 |
| Zr (de zer) | 10 | 6.160 | 0.201 | 5.80 | 6.40 |
| opaqued Ti (de opa) | 10 | 7.860 | 0.212 | 7.40 | 8.10 |
Thus, titanium abutments showed clinically unacceptable color changes compared to zirconia abutments, which demonstrated more natural color values (difference > 3.5). Titanium abutments opaqued with opaquer were clinically acceptable compared to standard titanium abutments (difference < 3.5).
3.1.2. Laboratory Statistics
The Kolmogorov-Smirnov normality test (Table 6) showed p-values > 0.05, indicating non-normality. Therefore, a non-parametric Kruskal-Wallis Test was performed.
| One-sample Kolmogorov-smirnov Test | ||
|---|---|---|
| Shade | Index | Group |
| 10 | N | de metal |
| 0.224 | Test Statistic | |
| 0.168 | Asymp. Sig. (2-tailed) | |
| 10 | N | de zer |
| 0.257 | Test Statistic | |
| 0.06 | Asymp. Sig. (2-tailed) | |
| 10 | N | de opa |
| 0.189 | Test Statistic | |
| 0.2 | Asymp. Sig. (2-tailed) | |
• Kruskal-Wallis H = 25.986, df = 2, p-value = 0.000.
This confirmed significant differences between the groups (Table 7).
| Test Statistics | |
|---|---|
| Shade | - |
| 25.986 | Kruskal-Wallis H |
| 2 | Df |
| 0.000 | Asymp. Sig. |
Pairwise comparisons with the LSD test (Table 8) revealed significant differences between all groups (p-value < 0.05).
Table 7 presents descriptive statistics of ∆E values across the three groups.
| Sig. | Mean Difference (I-J) | (J) Group | (I) Group |
|---|---|---|---|
| 0.000 | 3.610* | de zer | de metal |
| 0.000 | 1.910* | de opa | |
| 0.000 | -1.700* | de opa | de zer |
3.2. Clinical Results Clinical Sample Size Calculation
Sample size was estimated using G*Power 3.1.9.4. With an effect size of 0.5, an error of 0.05, and a power of 0.95, the sample size was deemed adequate (Fig. 13).
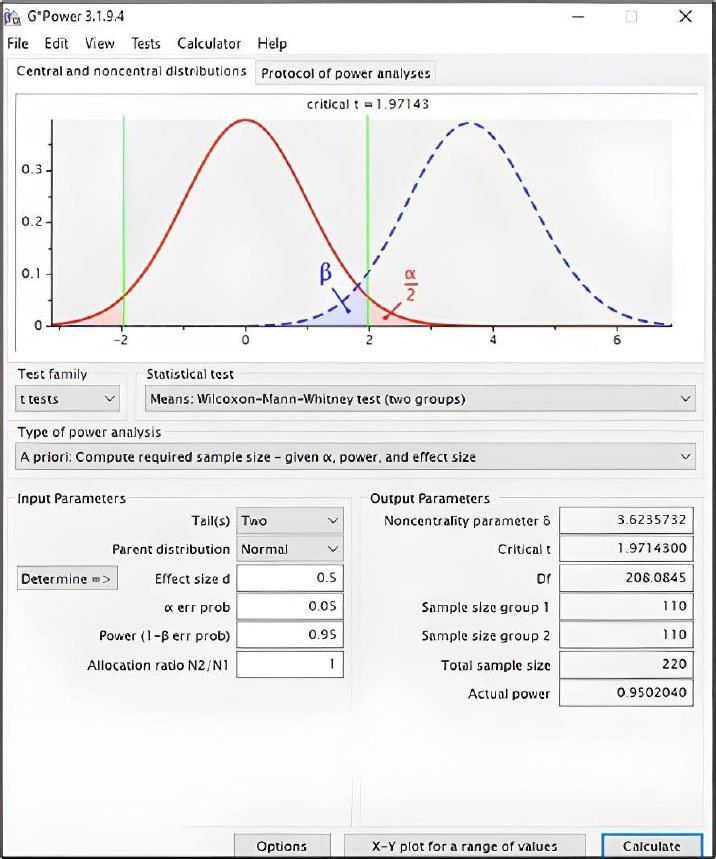
Determining the effect size value and the statistical power of the clinical study sample.
3.2.1. Clinical Findings
Tables 9 and 10 shows ∆E values for lithium disilicate crowns on zirconia abutments (n=8) and lithium disilicate crowns on opaqued titanium abutments (n=8).
| Crown | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| ∆E | 5.0 | 5.3 | 4.9 | 5.1 | 4.7 | 5.1 | 5.3 | 4.9 |
| Crown | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| ∆E | 6.9 | 7.1 | 6.8 | 6.9 | 7.2 | 7.1 | 7.3 | 7.0 |
3.2.2. Clinical Statistics
The comparative statistics between the two clinical groups show a statistically significant difference (p-value < 0.05) (Table 11).
| Group | N | Mean ∆E | Std | t | p-value |
|---|---|---|---|---|---|
| Zirconia abutments | 8 | 5.04 | 0.206 | -21.22 | 0.000 |
| Opaqued ti abutments | 8 | 7.04 | 0.166 | - | - |
3.2.3. Patient Satisfaction
A patient questionnaire assessed satisfaction with crown esthetics (shade and appearance):
- Patient 1: No difference between the two abutment types.
- Patient 2: No difference.
- Patient 3: Crowns on zirconia abutments looked more esthetic.
- Patient 4: No difference.
In summary, most patients reported no perceptible esthetic difference between the two types of abutments.
4. DISCUSSION
4.1. Discussion of the Laboratory Study and Materials
4.1.1. Rationale for Selecting the IPS e.max System
The IPS e.max system is a metal-free, glass-ceramic restorative material fabricated using CAD/CAM technology. Its strongest and most durable component is lithium disilicate, which also demonstrates the highest translucency compared to other high-strength ceramics. This system offers a wide range of translucency levels, and single restorations fabricated from lithium disilicate have shown high survival rates, particularly in the esthetic zone [35].
Crowns made from this material exhibit excellent marginal adaptation and long-term color stability. However, lithium disilicate crowns are also more prone to color changes and are influenced by the shade of the underlying abutment [36].
Previous studies have noted the appearance of a grayish hue when pure ceramic crowns are placed over titanium abutments. While dental technicians may compensate through internal characterization using layering techniques, this requires high skill and training, and results are inconsistent when the ceramic thickness is limited.
Therefore, this study sought to establish a standardized abutment–crown combination capable of achieving natural shade outcomes. Zirconia abutments with a titanium base were selected due to their favorable esthetic and mechanical properties [37]. Additionally, titanium abutments coated with opaquer were tested, since previous studies suggested that opaquer could mask the metallic hue while also being more affordable and widely available than zirconia [38].
To neutralize the influence of cement shade, pure glycerin-owing to its translucency-was used during the laboratory phase [39].
4.2. Discussion of Laboratory Findings
Color difference values (ΔE) smaller than 1 are imperceptible to the human eye. Values between 1 and 3.5 can only be detected by dental specialists or colorimeters and are thus considered clinically acceptable. Values above 3.5 are visible to the naked eye and deemed clinically unacceptable [34].
The ΔE of 9.7 for the titanium group far exceeds the clinical acceptability threshold (ΔE > 3.5), unequivocally confirming its unsuitability for esthetic anterior restorations with lithium disilicate crowns. In contrast, the zirconia group (ΔE = 6.1) and the opaqued titanium group (ΔE = 7.8) produced results that, while still perceptible, fall into a range that can be considered a significant aesthetic improvement. The superior performance of zirconia can be directly attributed to its high intrinsic whiteness and excellent light-scattering properties, which effectively mask the dark titanium base beneath.
Previous literature indicated that ∆E outcomes of lithium disilicate crowns vary depending on:
1. The abutment material.
2. The optical properties of the luting cement.
3. The thickness of the ceramic crown.
In this study, the influence of cement and crown thickness was standardized, leaving only the abutment material as the studied factor. Findings confirmed that titanium abutments induced clinically unacceptable color changes, while zirconia abutments with a titanium base achieved natural shade simulation. Titanium abutments opaqued with opaquer produced clinically acceptable outcomes.
These differences can be attributed to material properties: zirconia is a white material with high radiopacity, low absorption coefficient, and high density (residual porosity <0.05%), which effectively masks underlying discolored abutments [4]. Its high refractive index causes incident light to scatter and reflect rather than transmit, efficiently concealing the metallic hue beneath.
In contrast, opaqued titanium abutments produced greater ∆E values than zirconia abutments, possibly due to the manual application of opaquer, which requires technical expertise and should not exceed 0.1 mm in thickness. Inadequate coverage may compromise esthetic outcomes.
4.3. Comparison with Previous Studies
Our findings align with Köroğlu et al. (2016) [40], who reported that lithium disilicate crowns on titanium abutments were esthetically unacceptable, whereas zirconia-based abutments yielded favorable shade outcomes.
Similarly, our findings agree with those of Gehrke et al. (2024) [41], who reported that opaqued titanium abutments under lithium disilicate crowns could achieve clinically acceptable results compared to titanium abutments alone.
However, our results differ from those of Jirajariyavej et al. (2018) [42], who found no significant color difference between zirconia (white and yellow) and titanium abutments. This discrepancy may be attributed to their use of thicker lithium disilicate discs, which could effectively mask the underlying abutment color.
4.4. Discussion of the Clinical Study and Materials
In addition to the materials used in the laboratory phase, the clinical phase employed Variolink N (Ivoclar Vivadent), a dual-cure resin cement with a transparent shade, which is considered a permanent luting cement for implant crowns due to its esthetic advantages. It also received the Dental Advisor Award in 2010 (Almehmade et al., 2019) [43].
4.4.1. Discussion of Clinical Findings
- Group 1 (zirconia abutments): mean ∆E = 5.03
- Group 2 (opaqued titanium abutments): mean ∆E = 7.03
The difference between groups (ΔE = 2) is below the clinical threshold (3.5), meaning that the difference is detectable only with colorimeters or by dental specialists and is not visible to the naked eye.
Patient satisfaction results (n = 4):
- Three patients reported no noticeable difference between the two groups.
- One patient (a 23-year-old professional photographer) preferred zirconia abutments, likely due to the higher esthetic demands associated with her profession and age.
Although the clinical ΔE for the opaqued titanium group (7.03) was statistically higher than that of the zirconia group (5.03), the intergroup difference of 2.0 is below the clinical acceptability threshold of 3.5. This statistical finding is corroborated by the patient satisfaction survey, in which 3 out of 4 patients reported no discernible difference between the two abutment types. This convergence of quantitative and qualitative data strongly suggests that both zirconia and opaqued titanium abutments are clinically viable esthetic solutions, with the choice potentially being guided by factors such as cost, technical expertise, and specific case requirements.
5. STUDY LIMITATIONS
This study has several limitations that should be acknowledged. The clinical evaluation was conducted with a small sample size and lacked long-term follow-up, limiting the generalizability of the findings and the assessment of color stability over time. Furthermore, the in vitro conditions, while controlled, utilized glycerin as a simulated luting agent, which does not fully replicate the optical properties of clinical resin cements. The esthetic outcome for the opaque-coated group was also contingent upon a manual application technique, introducing a potential variable dependent on technical skill. Finally, the study was restricted to three specific abutment types and did not evaluate other available materials or designs.
CONCLUSION
This study demonstrates that the abutment substrate significantly influences the final color of lithium disilicate crowns in the esthetic zone. Under controlled in vitro conditions, conventional titanium abutments resulted in clinically unacceptable color changes (ΔE > 3.5), confirming their potential to compromise esthetics. Both zirconia abutments with a titanium base and opaque-coated titanium abutments served as effective alternatives, producing significantly lower and clinically acceptable ΔE values.
These laboratory findings were substantiated clinically, where no perceptible difference in color was reported by most patients between zirconia and opaque-coated titanium abutments, despite a statistically significant difference in colorimeter measurements. Therefore, from a purely esthetic standpoint, both options are valid for restoring anterior implants with lithium disilicate crowns.
The choice between them can be guided by non-esthetic considerations: zirconia abutments may be preferred for their inherent optical properties, while opaque-coated titanium abutments present a more cost-effective and technically straightforward solution. Based on these results, both are recommended over unmodified titanium abutments for superior esthetic outcomes. Future research should focus on the long-term color stability of these solutions and the impact of different clinical variables, such as luting cement shades and peri-implant soft tissue dynamics.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: M.M. Study conception design; Data collection; M.M. and N.B. Analysis and interpretation of results; N.S. Manuscript drafting. All authors reviewed the results and approved the final version of the manuscript.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
Ethical approval was obtained from Tishreen University, Iran (Approval No. 486, Session 8, February 4th, 2019).
HUMAN AND ANIMAL RIGHTS
All human research procedures followed were in accordance with the ethical standards of the committee responsible for human experimentation (institutional and national), and with the Helsinki Declaration of 1975, as revised in 2013.
CONSENT FOR PUBLICATION
Written informed consent was obtained, and each patient signed an authorization form.
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article is available in the [Zenodo] at [https://doi.org/10.5281/ zenodo.20549092].
ACKNOWLEDGEMENTS
Declared none.

