All published articles of this journal are available on ScienceDirect.

Antibacterial, Antibiofilm, Anti-adherence Activity, and Cytotoxicity Assay of Different Green Tea (Camellia sinensis) Extract Concentrations on Dental Pathogens: Aggregatibacter Actinomycetemcomitans and Streptococcus Mutans: An In Vitro study
Authors Info & Affiliations
Abstract
Introduction
This in vitro study aimed to assess the antibacterial, cytotoxicity, and anti-adherence properties of Camellia sinensis extracts (Green tea extract) against two dental pathogens associated with periodontal disease and dental caries, Aggregatibacter actinomycetemcomitans and Streptococcus mutans, respectively.
Methods
The minimal inhibitory concentration and anti-biofilm (anti-adherence) activity of different concentrations of green tea were determined using standard microbiological methods. The standard well diffusion was used to test for antibacterial activity. The biocompatible property of the selected concentrations on L929 fibroblast cells was tested using the MTT assay method.
Results
Among the different test concentrations of green tea, the growth of both test organisms was significantly inhibited at 500 µg/ml. Anti-biofilm concentrations of green tea extracts against both test organisms were found to be 300µg/ml. Antibacterial activity of selected concentrations showed significant inhibitory zones against Aggregatibacter actinomycetemcomitans and Streptococcus mutans when compared to standard antibiotics. During the MTT assay, no cytotoxicity was observed at any of the three test concentrations of green tea extracts. The concentration of 10µg/ml showed a maximum cell viability of 94.6 ± 0.57%, which was closest to control cell numbers. The test concentrations also had an antiadhesion effect on the tested bacteria.
Discussion
The study shows the positive antimicrobial activity of Green Tea (GT) extracts against Streptococcus mutans and Aggregatibacter actinomycetemcomitans, which correlates with earlier studies. Furthermore, it shows that GT extract has antiadhesion potential and further has no cytotoxic effects on normal fibroblast cells, indicating GT's potential for oral health applications.
Conclusion
The results show that green tea has a positive deterrent effect on biofilm formation and can be used as an additive in herbal formulations; however, further research is necessary.
1. INTRODUCTION
Dental caries is a prevalent chronic infectious microbial but preventable oral disease caused by the phasic demineralisation of dental hard tissues due to a sugar-driven dysbiosis of the dental biofilm microbiome. Over 2 billion people worldwide suffer from permanent tooth caries, and 514 million children have primary tooth caries. The condition disproportionately affects people from lower socioeconomic backgrounds [1, 2].
Streptococcus mutans is a facultative aerobic Gram‐positive bacterium and is a significant contributor to the development of dental caries. It has also been found to be a primary etiological agent of dental caries [3, 4]. Streptococcus mutans produces dental biofilm formation along with other biofilm-colonising bacteria [5]. It produces an extracellular enzyme, glucosyltransferase-B, which converts glucan from sucrose present in food substances [6]. Moreover, its production of lactic acid further solidifies its role as a significant cause of dental caries. Currently, it is also a suspect in systemic diseases and infections as well.
Periodontitis is a common, multifactorial inflammatory disease that results in progressive, irreversible periodontal attachment loss, alveolar bone loss, and concurrent tooth loss. It is primarily caused by periodontopathic bacteria that grow in a dental biofilm on the surfaces of tooth roots [7]. This chronic inflammatory disease is also thought to be caused by an interaction between the hyperactive host immune system and the dysbiotic bacterial microbiome, rather than just an increase in the number of bacteria. A shift toward an increase in Gram-negative anaerobic periodontopathic bacteria, such as Aggregatibacter actinomycetemcomitans, is another indication of this dysbiotic state. Therefore, individuals with periodontitis are often found to have higher levels of these periodontopathogens. Furthermore, studies have demonstrated that periodontal therapy may reduce the population of periodontopathic bacteria, although it might not completely eliminate them [8–10].
Aggregatibacter actinomycetemcomitans is a Gram-negative bacterium that lives in the mouth and is part of the normal oral microbiota. Its potent antigenic profile makes it play a role in the formation of dental biofilm and periodontal disease [11]. Infective endocarditis is an infection of the heart's lining, primarily impacting the valves. It results when subendothelial tissue erodes and is exposed to the bacteria [11, 12]. Aggregatibacter actinomycetemcomitans has been demonstrated to induce infective endocarditis in adults with inadequate dental health and preexisting valvular heart disease [11, 12]. Additionally, Streptococcus mutans, the primary cariogenic bacterium, and Aggregatibacter actinomycetemcomitans, a periodontopathic bacterium, are recognised for their ability to upregulate cytokines and induce inflammation in periodontal host tissues [13, 14]. These bacteria hold substantial importance regarding oral health, as they are linked to both dental caries and periodontal diseases, potentially compromising an individual's systemic health. Consequently, it is essential to identify and develop potential antimicrobials that could be used to target these bacteria in dental biofilm and reduce the bacterial load in the oral cavity [15].
The conventional oral-care arsenal includes antibiotics, antiseptics, biocides, fluoride, iodine compounds, quaternary ammonium salts, and surfactants, which can be cytotoxic and may not eradicate oral biofilms [16]. This has led to the exploration of plant-derived or natural compounds as complementary or alternative strategies, many of which have been shown to combat dental biofilms [17–19]. Moreover, antibiofilm therapy with herbal products has regained considerable interest, as they are considered safer, overcome the development of multi-resistant bacteria, are less expensive, and have no adverse effects [20]. Therefore, the search for natural plant compounds as an alternative to existing oral disinfectants is meaningful.
Green Tea (GT) is made from the leaf of the plant “Camellia sinensis” and has been studied for its various properties and effects. GT is reported to contain various bioactive substances, including catechins, which have demonstrated great potential for having antimicrobial effects [21]. Additionally, studies have also revealed that the bioactive compounds present in GT have an immunomodulatory effect [22]. Moreover, GT (Camellia sinensis) contains four principal catechins, namely epicatechin (EC), epicatechin gallate (ECG), epigallocatechin (EGC), and epigallocatechin gallate (EGCG) [23]. According to Hengge (2019), cariogenic and chronic wound-infection biofilms appeared to be advantageous targets for EGCG. In addition, EGCG also plays a significant role by targeting the glucosyltransferase enzyme in charge of converting sucrose to the glucan present in the food [24]. Hence, it is noted to have significant anti-inflammatory and anticarcinogenic potential.
Prior studies have not investigated the anti-adhesion and cytotoxic effects of green tea extracts. Furthermore, green tea sourced from the Coimbatore region in Tamil Nadu, India, has not been evaluated for its impact on the bacteria under investigation. Hence, with this background context, the study aims to determine the antibacterial and anti-adhesion properties of GT (Camellia sinensis) extracts against Aggregatibacter actinomycetemcomitans and Streptococcus mutans.
2. MATERIALS AND METHODS
2.1. Procurement and Extraction of GT (Camellia Sinensis)
GT leaf powder was obtained from the farmhouse at Tamil Nadu Agricultural University, Coimbatore, Tamil Nadu, India (11.055303566545515, 76.92992803327184). The Soxhlet apparatus was used to procure solvent extracts of the leaf powder using ethanol. The collected extracts were individually transferred to petri dishes and oven dried at 50°C; subsequently, the extracts were scraped and stored in airtight brown amber containers at room temperature (Fig. 1a and b).
a. Dried GT leaf powder b. GT extract.
2.2. Procurement of Test Bacteria-streptococcus Mutans and Aggregatibacter Actinomycetemcomitans
Test organisms that were highly significant and had etiological characteristics associated with dental biofilm formation were selected for the study. Gramme Positive Lab, Coimbatore, India, our testing facility, supplied pertinent bacterial strains for the chosen bacteria, Streptococcus mutans ATCC 25175 and Aggregatibacter actinomycetemcomitans b. The strains had previously been in use at the testing facility and were obtained from Himedia Labs in Thane, India.
2.3. Minimal Inhibitory Concentration of GT Extracts
Resazurin (270 mg) was dissolved in 40 millilitres of sterile distilled water to prepare for the assay. A vortex mixer was employed to ensure that the mixture was uniform and thoroughly dissolved. The experiment was conducted in aseptic conditions in a 96-well plate. A 96-well plate was marked sterile. First, a 100μL volume of various sample solution concentrations (1000, 500, 250, 125, 62.5, 31.2, 15.6, and 7.8 μg/mL) of Dimethyl Sulphoxide (DMSO) was pipetted into the plate well. Subsequently, 50μL of nutrient-rich broth was introduced into each well and diluted. Ten microlitres (μL) of resazurin indicator solution was added to each well. Following this, each well received the addition of 10μL of bacterial suspension [25].
As a standard control, streptomycin (7.8, 15.6, 31.2, 62.5, 125, 250, 500, 1000μL/mL) was employed. Each plate was covered securely with cling material to prevent bacteria from drying out. The plate was subsequently incubated at 37°C for 18 to 24 hours, after which the colour change was visually observed. Positive colour changes were those that went from blue to pink or colourless, while negative colour changes were those that did not occur. The Minimal Inhibitory Concentration (MIC) value of the sample was determined by observing a colour change at the lowest possible concentration. An ELISA reader was used to measure the plate's absorbance at 600 nm.
The following formula (1) was used to calculate the percentage of inhibition:
% of Inhibition = Control- Test/Control*100 –...(1)
2.4. Antibacterial Evaluation of GT Extracts
The antibacterial efficacy of GT extracts was evaluated against the test organisms, Aggregatibacter actinomycetemcomitans and Streptococcus mutans, utilising the well-diffusion method [25]. All test cultures were inoculated with a sterile nutrient broth (g/L) containing 5 grams of peptone, 5 grams of yeast extract, 3 grams of beef extract, 5 grams of sodium chloride, and a final pH of 7.0 ± 0.2 The cultures were left to incubate for 24 to 48 hours. Sterile Mueller-Hinton Agar (MHA) plates were prepared and allowed to solidify. Swabs were used to evenly spread 0.1% inoculum suspensions of the test organism on the agar surface in each case. The agar surface of each plate was cut into 6-mm wells while keeping the area sterile. The wells received an addition of the chosen MIC concentration of GT extracts (20 µg/ml and 30 µg/ml). Normal streptomycin, on the other hand, was added at a rate of 4 µg/ml. DMSO was employed as a negative control. Following a 24-hour incubation at 37°C, the plates were assessed for significant zones of inhibition. All tests were performed three times to obtain mean and standard deviation values, and the sample values were statistically compared with the standard drug.
2.5. Anti-biofilm Activity of GT Extracts
The bacterial ability to form biofilms was assayed with minimal modifications of the method described by O’Toole and Kolter (1998) [26]. Fifty microliters of fresh bacterial suspension were added to sterile 96-well tissue culture plates that were filled with 100μl of nutrient broth each. To the standard test, 100μl of the standard solution (Streptomycin 1 mg/ml) was added. The GT extract was added in test wells ranging from 20 to 100μg/ml. The contents of each well were carefully removed by tapping the plates after a 24-hour incubation at 37°C. The wells were washed with 200 μL of sterile saline to remove any non-adherent microorganisms. After 20 minutes of room temperature incubation, the biofilm that adherent cells formed in the plate was dyed with 0.1% crystal violet. After thoroughly cleaning the excess stain with deionized water, 200μl of 96% ethanol was used to fix the plates. With the aid of an ELISA microplate reader, the Optical Densities (OD) of stained adhering bacteria were determined at 630 nm.
2.6. Anti-adherence Activity
Test tubes containing 0.37 grams of dehydrated culture media, which constituted Brain Heart Infusion (BHI) broth and 10% sucrose, were filled with nine millilitres of each GT extract [27]. Subsequently, standardised glass specimens with a diameter of 2 mm and a length of 5 cm were inserted in these tubes and autoclaved. One millilitre of 24-hour test cultures (Aggregatibacter actinomycetemcomitans and Streptococcus mutans) was added to each tube and then incubated for ninety minutes at 37°C to assess how well the bacteria adhered to the surface. Then, during the incubation period, the glass specimens were transferred into tubes containing pH 7.2 buffered phosphate saline. In place of GT extract samples, distilled water was used in a similar experimental setup using a different set of tubes. After shaking the test and control tubes, sterile NaCl (0.85%) saline solution was used to make 10-1 and 10-2 dilutions from the original suspension. BHI agar was then divided into 0.1 ml aliquots of each dilution and put in an incubator at 37°C for 48 hours. After this time frame, the log CFU/ml value was computed, and the number of colonies was counted [15].
2.7. Cytotoxicity Assay of GT Extracts – MTT Assay
The biocompatibility of Camelia sinensis (GT) extracts used in the study to assess their antibacterial and anti-adherence activities against test organisms was evaluated using the MTT assay [28]. To achieve confluent cell growth, 12-well microtiter plates were used for cultivating L929 fibroblast cell lines. The created fibroblast monolayer received separate applications of the chosen GT extract sample (10µl, 20µl, and 30µl). For two hours at 37°C in an incubator, the samples were mixed with 1 milliliter of Dulbecco's modified Eagle medium (DMEM) in 24-well plates. Following standard cell-culture procedures, 10,000 L929 fibroblast cells per well were seeded onto the plates. They were incubated at 37°C with 5% CO2 for fifteen days. Using the photometric MTT test, the impact of GT extracts on fibroblast viability was assessed. Samples from the 24-well plates were collected at each time point and transferred to fresh plates for the MTT assay. Each well received around 1 milliliter of MTT solution, and the plates were then incubated for 3 hours. To induce the development of purple crystals, 100µl of 70% isopropanol was used to rinse and desorb each well. The purple crystal-dyed solution was transferred to 96-well microtiter plates and measured at 550 nm after 40 minutes of agitation of the plates at 400 rpm/min. Cell viability was then expressed as a percentage of the control sample (100%).
3. RESULTS AND DISCUSSION
3.1. Minimal Inhibitory Concentration of GT Extracts
Minimal inhibitory concentration against Aggregatibacter actinomycetemcomitans was determined using a control and standard antibiotic (Fig. 2) (Table 1). Among the different test concentrations of GT extracts, the growth of the test bacteria was inhibited at 500 µg/ml compared with the standard streptomycin at 125 µg/ml. The growth inhibition percentage was also calculated. MIC of 500µg/ml inhibited 40.0%, and 125µg/ml of streptomycin inhibited 45.8% of Aggregatibacter actinomycetemcomitans. The inhibition percentage ranged from 10.5% to 47.6% across all GT extract concentrations, as presented in Table 1.
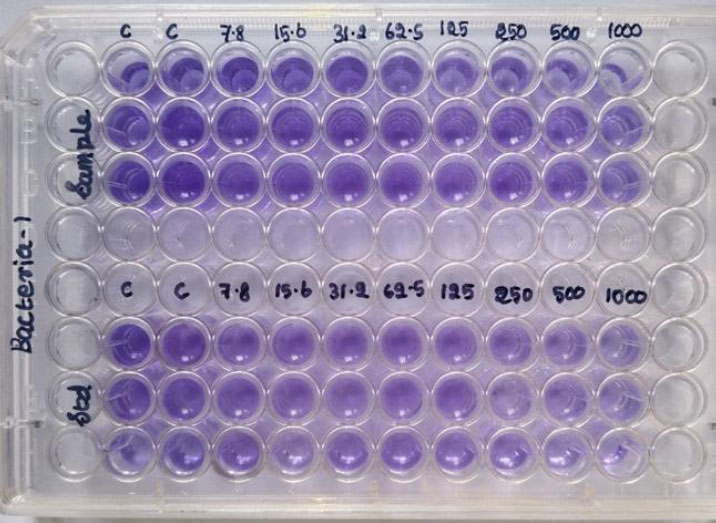
Minimal Inhibitory Concentration (MIC) (Microdilution assay) of GT against Aggregatibacter actinomycetemcomitans.
| S. No | Samples |
Concentration (µg/ml) |
Absorbance at 600nm | Mean | Growth Inhibition (%) | ||
|---|---|---|---|---|---|---|---|
| Test 1 | Test 2 | Test 3 | |||||
| 1 | Control (Growth) | - | 1.74 | 1.62 | 1.75 | 1.70 ± | - |
| 2 | GT(Camellia sinensis) | 7.8 | NE | NE | NE | NE | NE |
| 15.6 | NE | NE | NE | NE | NE | ||
| 31.2 | NE | NE | NE | NE | NE | ||
| 62.5 | NE | NE | NE | NE | NE | ||
| 125 | NE | NE | NE | NE | NE | ||
| 250 | 1.54 | 1.56 | 1.47 | 1.52 ± 0.57 | 10.5 | ||
| 500 | 0.98 | 1.14 | 0.96 | 1.02 ± 1.05 | 40.0* | ||
| 1000 | 0.86 | 0.95 | 0.88 | 0.89 ± 1.05 | 47.6 | ||
| 3 | Standard (Streptomycin) | 7.8 | - | - | - | - | - |
| 15.6 | 1.54 | 1.44 | 1.52 | 1.50 ± 0.75 | 11.76 | ||
| 31.2 | 1.42 | 1.32 | 1.34 | 1.36 ± 0.57 | 20.0 | ||
| 62.5 | 1.35 | 1.25 | 1.16 | 1.25 ± 0.57 | 26.4 | ||
| 125 | 0.85 | 0.96 | 0.95 | 0.92 ± 0.75 | 45.8* | ||
| 250 | 0.76 | 0.82 | 0.75 | 0.77 ± 1.05 | 54.7 | ||
| 500 | 0.64 | 0.6 | 0.62 | 0.62 ± 0.57 | 63.5 | ||
| 1000 | 0.58 | 0.52 | 0.48 | 0.52 ± 1.05 | 69.4 | ||
Note: *The percentage of growth inhibition for Camellia sinensis was found to be statistically significant, as a similar growth inhibition percentage for Streptomycin was found to be evident (p<0.05).
Minimal inhibitory concentration against Streptococcus mutans was determined using a control and standard antibiotic (Fig. 3) (Table 2). Among the different test concentrations of GT extracts, the growth of test bacteria was found to be inhibited at 500µg/ml when compared to standard streptomycin at 250µg/ml. The growth inhibition percentage was also calculated. MIC of 500µg/ml inhibited 34.5%, and 250µg/ml of streptomycin inhibited 50.6% of Streptococcus mutans. The inhibition percentage ranged from 6.17% to 46.2% for all the respective concentrations, as presented in Table 2.
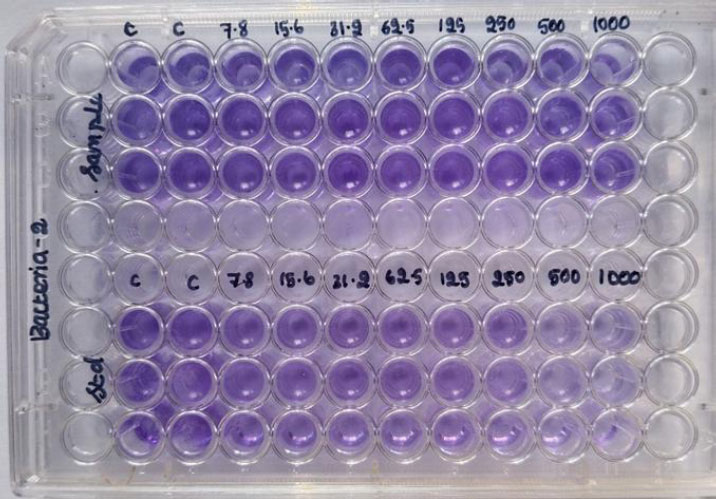
Minimal Inhibitory Concentration (MIC) (Microdilution assay) of GT extracts against Streptococcus mutans.
| S. No | Samples |
Concentration (µg/ml) |
Absorbance at 600nm | Mean | Growth Inhibition (%) | ||
|---|---|---|---|---|---|---|---|
| Test 1 | Test 2 | Test 3 | |||||
| 1 | Control (Growth) | - | 1.65 | 1.55 | 1.68 | 1.62 ± 0.57 | - |
| 2 | GT extracts | 7.8 | NE | NE | NE | NE | NE |
| 15.6 | NE | NE | NE | NE | NE | ||
| 31.2 | NE | NE | NE | NE | NE | ||
| 62.5 | NE | NE | NE | NE | NE | ||
| NE | NE | NE | NE | NE | NE | ||
| 250 | 1.56 | 1.48 | 1.53 | 1.52 ± 1.05 | 6.17 | ||
| 500 | 1.10 | 0.98 | 1.12 | 1.06 ± 0.57 | 34.5 | ||
| 1000 | 0.96 | 0.84 | 0.82 | 0.87 ± 1.05 | 46.2* | ||
| 3 | Standard (Streptomycin) | 7.8 | 1.55 | 1.48 | 1.54 | 1.52 ± 0.57 | 6.17 |
| 15.6 | 1.45 | 1.35 | 1.43 | 1.41 ± 0.75 | 12.9 | ||
| 31.2 | 1.38 | 1.25 | 1.32 | 1.31 ± 0.57 | 19.1 | ||
| 62.5 | 1.25 | 1.16 | 1.10 | 1.17 ± 0.75 | 27.7 | ||
| 125 | 0.98 | 0.88 | 0.92 | 0.92 ± 1.05 | 43.2 | ||
| 250 | 0.85 | 0.76 | 0.80 | 0.80 ± 1.05 | 50.6* | ||
| 500 | 0.73 | 0.65 | 0.58 | 0.65 ± 1.05 | 59.8 | ||
| 1000 | 0.65 | 0.58 | 0.52 | 0.58 ± 0.57 | 64.1 | ||
Note: *The percentage of growth inhibition for Camellia sinensis was found to be statistically significant, as a similar growth inhibition percentage for Streptomycin was found to be evident (p<0.05).
3.2. Antibacterial Activity of GT Extracts
The antibacterial activity of GT was evaluated using the standard agar well-diffusion method. During the analysis, substantial inhibitory zones were observed in both trial experiments (S1 and S2). The zones were close to the positive control streptomycin. No zones were found for the negative control (DMSO – dimethyl sulfoxide). Trial-1 (S1) showed inhibitory zones of about 17.3 ± 1.05 mm and 18.9 ± 0.57 mm against Aggregatibacter actinomycetemcomitans and Streptococcus mutans. Trial-2 (S2) showed inhibitory zones of about 17.9 ± 0.57 mm and 18.3 ± 1.05 mm against the respective organisms. In Table 3 and Fig. (4), the inhibitory zones against test bacteria are presented separately.
| S. No. | Test Organism | Zone of Inhibition (Millimetre) | |||
|---|---|---|---|---|---|
| S1 | S2 | Std | NC | ||
| 1 | Aggregatibacter actinomycetemcomitans | 17.3 ± 1.05 | 18.9 ± 0.57 | 21.3 ± 1.05 | 0 |
| 2 | Streptococcus mutans | 17.9 ± 0.57 | 18.3 ± 1.05 | 21.6 ± 0.75 | 0 |
Note: S1: Trial – 1, S2: Trial -2, PC: Positive control (Streptomycin), NC: Negative control (DMSO).
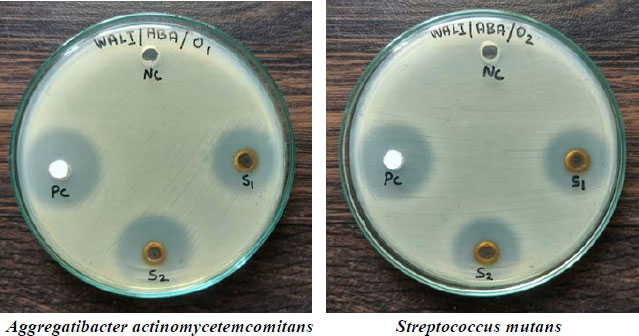
Antibacterial activity of GT(Agar disc diffusion method).
3.3. Anti-biofilm Assay of GT Extracts
The anti-biofilm or anti-adherence study was carried out using a modified protocol of O’Toole and Kolter (1998) [26]. Table 4 presents the antibiofilm activity of different GT extract concentrations against Aggregatibacter actinomycetemcomitans. In Fig. (5), the colour-uptaking ability of the test bacteria is shown. The colour reduction indicated the anti-biofilm efficiency of GT extract concentrations. Anti-biofilm concentration against test organisms was determined using a control of a standard antibiotic. Among the different test concentrations of Camellia sinensis, the growth of test bacteria was found to be inhibited significantly at 300µg/ml when compared to standard streptomycin at 30µg/ml. The growth inhibition percentage was also calculated. An anti-biofilm concentration of 300µg/ml inhibited 52.1% of Aggregatibacter actinomycetemcomitans. The inhibition percentage ranged from 3.68% to 67.3% for all the respective concentrations, as presented in Table 4.
| S. No | Samples |
Concentration (µg/ml) |
Absorbance at 600nm | Mean | Growth Inhibition (%) | ||
|---|---|---|---|---|---|---|---|
| Test 1 | Test 2 | Test 3 | |||||
| 1 | Control (Growth) | - | 1.94 | 1.86 | 1.92 | 1.90 ± 0.57 | - |
| 2 | GT extracts | 100 | 1.82 | 1.88 | 1.79 | 1.83 ± 0.57 | 3.68 |
| 200 | 1.36 | 1.34 | 1.29 | 1.32 ± 0.75 | 29.9 | ||
| 300 | 0.91 | 0.89 | 0.95 | 0.91 ± 1.05 | 52.1* | ||
| 400 | 0.72 | 0.78 | 0.71 | 0.73 ± 1.05 | 61.5 | ||
| 500 | 0.62 | 0.65 | 0.59 | 0.62 ± 1.05 | 67.3 | ||
| 3 | Standard (Streptomycin) | 10 | 1.85 | 1.82 | 1.86 | 1.84 ± 0.75 | 3.15 |
| 20 | 1.38 | 1.32 | 1.26 | 1.32 ± 0.75 | 30.5 | ||
| 30 | 0.94 | 0.9 | 0.88 | 0.90 ± 1.05 | 52.6* | ||
| 40 | 0.77 | 0.72 | 0.74 | 0.74 ± 0.75 | 61.0 | ||
| 50 | 0.64 | 0.59 | 0.58 | 0.60 ± 1.05 | 68.4 | ||
Note: *The percentage of growth inhibition for Camellia sinensis was found statistically significant, as a similar growth inhibition percentage for Streptomycin was found to be evident (p<0.05).

Anti-biofilm studies of GT extracts against Aggregatibacter actinomycetemcomitans using the modified protocol of O’Toole and Kolter.
Table 5 presents the anti-biofilm activity of GT at different test concentrations against Streptococcus mutans. In Fig. (6), the colour-uptaking ability of the test bacteria is presented. The colour reduction indicated the anti-biofilm efficiency of GT extract concentrations. The anti-biofilm concentration of the test organism was determined using a control and a standard antibiotic. Among the different test concentrations of GT, the growth of test bacteria was found to be inhibited significantly at 300µg/ml when compared to standard streptomycin at 30µg/ml. The growth inhibition percentage was also calculated. An anti-biofilm concentration of 300µg/ml inhibited 48.0% of Streptococcus mutans. The inhibition percentage ranged from 4.37% to 69.9% for all the respective concentrations, as presented in Table 5.
| S. No | Samples |
Concentration (µg/ml) |
Absorbance at 600nm | Mean | Growth Inhibition (%) | ||
|---|---|---|---|---|---|---|---|
| Test 1 | Test 2 | Test 3 | |||||
| 1 | Control (Growth) | - | 1.88 | 1.84 | 1.78 | 1.83 ± 0.57 | - |
| 2 | GT extracts (Camellia sinensis) | 100 | 1.75 | 1.72 | 1.8 | 1.75 ± 0.75 | 4.37 |
| 200 | 1.28 | 1.32 | 1.29 | 1.29 ± 0.57 | 29.5 | ||
| 300 | 0.92 | 0.99 | 0.94 | 0.95 ± 1.05 | 48.0* | ||
| 400 | 0.68 | 0.62 | 0.67 | 0.65 ± 1.05 | 64.4 | ||
| 500 | 0.55 | 0.59 | 0.53 | 0.55 ± 1.05 | 69.9 | ||
| 3 | Standard (Streptomycin) | 10 | 1.76 | 1.72 | 1.69 | 1.72 ± 0.75 | 6.01 |
| 20 | 1.25 | 1.19 | 1.27 | 1.23 ± 0.57 | 32.7 | ||
| 30 | 0.90 | 0.96 | 0.94 | 0.93 ± 1.05 | 49.1* | ||
| 40 | 0.71 | 0.69 | 0.74 | 0.71 ± 1.05 | 61.2 | ||
| 50 | 0.58 | 0.56 | 0.62 | 0.58 ± 1.05 | 68.3 | ||
Note: *The percentage of growth inhibition for Camellia sinensis was found to be statistically significant, as a similar growth inhibition percentage for Streptomycin was found to be evident (p<0.05).
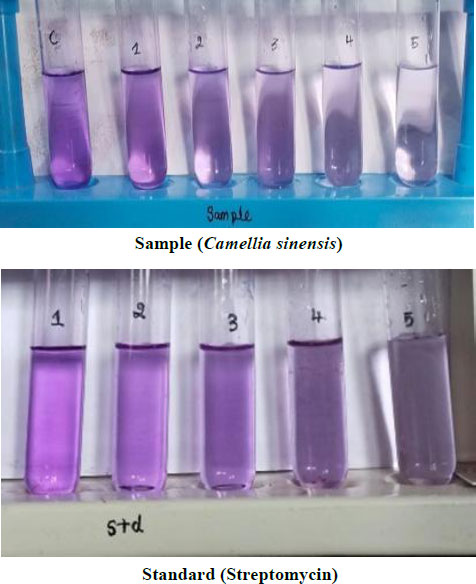
Anti-biofilm studies of GT against Streptococcus mutans using the modified protocol of O’Toole and Kolter.
3.4. Adherence Test
Adherence test results indicated that GT extract samples markedly diminished the quantity of organisms, Streptococcus mutans and Aggregatibacter actinomycetemcomitans, adhering to the glass specimens [27]. However, the samples that were exposed to distilled water had more bacterial colonies on BHI agar plates than the samples that were exposed to GT extract. In Figs. (7 and 8), the difference in the number of bacterial colonies for Streptococcus mutans and Aggregatibacter actinomycetemcomitans is presented, respectively.

Number of colonies observed on BHI agar plates (Streptococcus mutans).

Number of colonies observed on BHI agar plates (Aggregatibacter sp).
We calculated and showed the log CFU/ml for each experimental group after 90 minutes of contact between Streptococcus mutans and Aggregatibacter actinomycetemcomitans with the test solutions.
Trial-1 and Trial-2 against Streptococcus mutans yielded 2.3 X 104 CFU/ml and 2.8 X 104 CFU/ml, respectively; in contrast, the cultures exposed to distilled water exhibited a greater colony count of approximately 8.7 X 104 CFU/ml (Fig. 9).
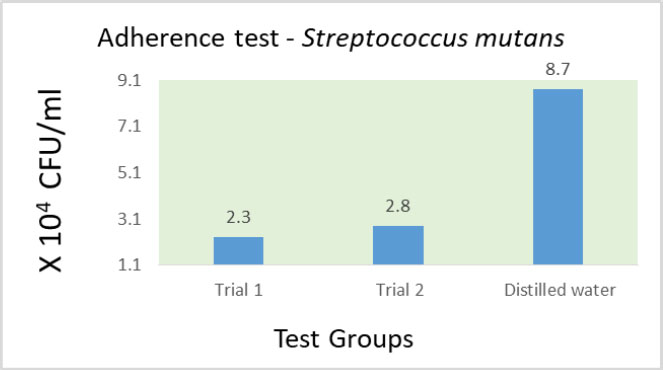
Mean (log of CFU/ml) obtained in the analysis of bacterial adherence to glass (Streptococcus mutans).
In a separate test, Trial-1 and Trial-2 against Aggregatibacter actinomycetemcomitans yielded 3.4 X 104 CFU/ml and 3.9 X 104 CFU/ml, respectively. The cultures that were exposed to distilled water had more colonies of about 9.2 X 104 CFU/ml (Fig. 10).
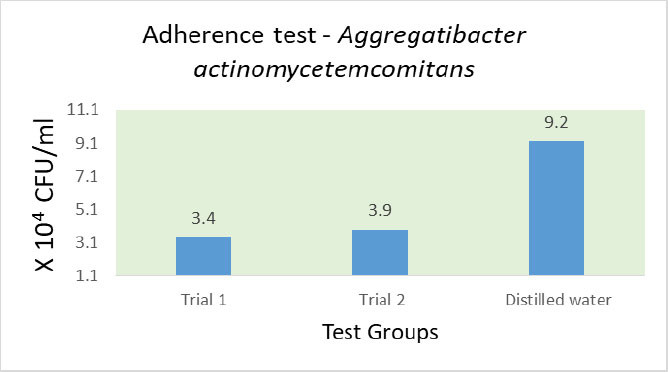
Mean (log of CFU/ml) obtained in the analysis of bacterial adherence to glass (Aggregatibacter actinomycetemcomitans).
The CFU/ml values obtained for the sample and distilled water against the test organisms demonstrated that the GT extract significantly impeded the adherence of microorganisms to the surface of the glass specimen.
3.5. MTT Assay of GT Extract
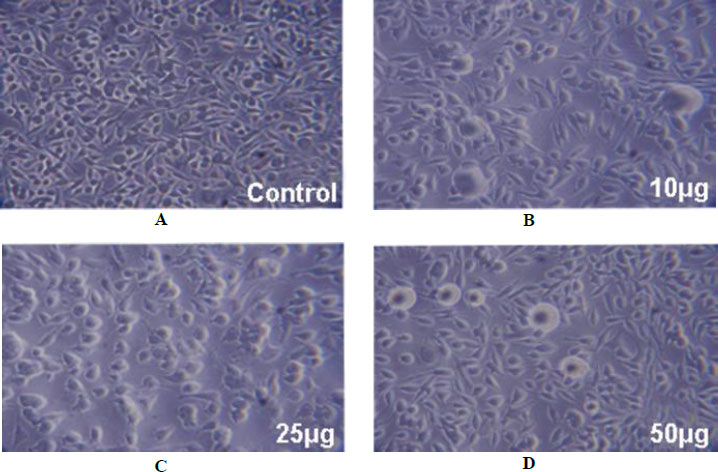
In the present study, the standard MTT assay was used to assess the cytotoxic effects of the GT extract. The activity was assayed in confluent L929 fibroblast cells at different concentrations of GT extracts. During the study, no cytotoxicity was observed, and the images are presented in Fig. (11), compared with control samples. Among the three different concentrations, 10µg /ml showed a maximum cell viability of 94.6 ± 0.57%, which was closest to control cell numbers (Table 6). The other two concentrations also showed more than 90% cell viability, indicating no cytotoxicity for the GT extract used in the study. These results show that these specified concentrations could be appropriate as an additive in herbal formulations and in further research against dental caries and periodontal-associated infections.
MTT assay of GT concentrations.
11A – Control; 11B – Cells treated with 10µg/ml of GT extracts; 11C – Cells treated with 25µg/ml of GT extracts; 11D – Cells treated with 50µg/ml of GT extracts Magnifications – 40X and 100X.
| S. No. | Fibroblast Cell Lines – MTT Assay | Cytotoxic Reactivity | ||
|---|---|---|---|---|
|
Concentration (µg) |
Cytotoxicity (%) | Cell viability (%) | ||
| 1 | Control | 0 | > 99 | No cytotoxicity |
| 2 | 10 | 5.3 ± 1.05 | 94.6 ± 0.57 | No cytotoxicity |
| 3 | 25 | 7.6 ± 0.75 | 92.3 ± 0.75 | No cytotoxicity |
| 4 | 50 | 9.3 ± 1.05 | 90.6 ± 0.57 | No cytotoxicity |
The obtained results were found to be consistent with those of other research works identified in the literature review. Furthermore, published scientific literature was also found to be supportive of this concept, illustrating the significance and possible uses of different bioactive compounds of GT, including its anticancer properties, antimicrobial properties, and antioxidant properties. Therefore, we present the findings of our current study below and compare them with the existing scientific literature.
Araghizadeh et al. (2013) studied the inhibitory activity of GT extract (50 to 1.56mg/ml) against clinically isolated periodontopathic (Porphyromonas gingivalis and Prevotella intermedia) and cariogenic bacteria (Aggregatibacter actinomycetemcomitans, and Streptococcus mutans). Agar disc diffusion and broth microdilution assays were determined [29]. The results showed that S. mutans were sensitive to GT extract at concentrations of 6.25, 12.5, 25, and 50mg/ml, producing bacterial inhibition zones that ranged from 10 to 38mm. The MIC of GT extract for S. mutans was 3.28mg/ml, and for A. actinomycetemcomitans, it was 6.25 mg/ml. The results of our study also showed that GT extracts had an antibacterial effect against Streptococcus mutans and Aggregatibacter actinomycetemcomitans.
In another study by Anita et al. (2014), the MIC against S. mutans was 18.33 mm for 30 μl containing 300 μg of ethanolic GT extract [30]. The results of this present study also showed similar results.
Research has also shon that EGCG has potent antibacterial properties. The most prevalent catechin in GT, EGCG, has been linked to its antibacterial properties [31, 32]. Additionally, Saito et al. (2012) noted that Aggregatibacter actinomycetemcomitans lipopolysaccharide's cytotoxic effects on cells were significantly inhibited by ECG and EGCG [33]. The results of our study are in conciliation with the results of a recent study on GT extract, which indicated that GT extracts had considerable effects on salivary Streptococcus mutans levels compared with CHG [34]. In our present study, GT extracts showed a fair amount of antimicrobial activity against both periodontopathic bacteria, Aggregatibacter actinomycetemcomitans, and cariogenic bacteria, Streptococcus mutans. Hence, we suggest, similar to Tafazoli and Moghadam (2020) and Sharma et al. (2023), that GT can be used as a regular reinforcement to routine dental hygiene practices and can be used as an additive to oral hygiene products [35, 36]. Furthermore, it is postulated that the antibacterial activity of the GT extract on Streptococcus mutans and A. actinomycetemcomitans is due to the presence of bioactive compounds and their low-toxicity characteristics [37].
The results of the MTT assay of our present study showed that the GT extract had no cytotoxic effect on the tested normal fibroblast cells, which is similar to what Esghaei et al. found. They found that GT extracts had considerable inhibitory effects on colorectal cancer cell lines while having little effect on normal L929 fibroblast cells [38]. Moreover, the extracts have also been shown to have apoptotic effects on other cancer cell lines [39, 40]. The present study also found that GT extracts inhibit bacterial adhesion to glass. This phenomenon can also explain its antibiofilm characteristics.
Catechins function as both direct and indirect modulators of signalling pathways that govern inflammation, cellular proliferation, and stress responses. A recurrent theme in various studies is that catechins, particularly epigallocatechin gallate (EGCG), inhibit pro-inflammatory signalling pathways (NF-κB, MAPKs) and pro-survival and pro-growth pathways (EGFR, PDGF receptor, STAT3), consequently diminishing the production of inflammatory mediators and cell proliferation. These functions are facilitated via direct interactions with membrane proteins, modulation of kinase activities, and regulation of transcription factors, rather than exclusively through antioxidant activity [41, 42]. Thus, catechin-mediated inhibition pathways may have different ways of profoundly modulating various anti-inflammatory and stress responses.
4. STUDY LIMITATIONS
This study did not include the separation and analysis of different phytochemicals in Camellia sinensis. Furthermore, it was restricted to analysing green tea and did not examine processed teas, such as black tea. The research also did not include molecular docking analysis, which could be explored in future studies. Additional research could investigate the effects of Camellia sinensis on other oral pathogenic bacteria.
CONCLUSION
The antibacterial and anti-biofilm properties of GT extracts against dental pathogens, Aggregatibacter actinomycetemcomitans and Streptococcus mutans, were investigated. Among the different test concentrations of GT, the growth of both test organisms was significantly inhibited at 500µg/ml. Anti-biofilm concentrations of GT extracts against both test organisms were found to be 300µg/ml. Antibacterial activity of selected concentrations showed significant inhibitory zones against Aggregatibacter actinomycetemcomitans and Streptococcus mutans when compared to standard antibiotics. During the MTT assay, no cytotoxicity reactions were observed for all three test concentrations of GT extracts, with 10µg/ml showing maximum cell viability of 94.6 ± 0.57%, which was closest to control cell numbers. The strong and potent antibacterial constituents (catechin, epigallocatechin gallate, and galloyl moieties) present in GT extracts were proven to be natural anti-cariogenic agents. The results of our study further elucidate the positive deterrent effect of GT on dental pathogens and dental biofilm formation and adhesion. In addition to its antibacterial effects, its anti-adhesive properties make it a promising natural agent that can be employed for the prevention and management of oral diseases. However, additional research and clinical trials are necessary to fully understand the mechanisms and optimise the use of GT in herbal formulations for dental care.
AUTHORS’ CONTRIBUTIONS
It is hereby acknowledged that all authors have accepted responsibility for the manuscript's content and consented to its submission. They have meticulously reviewed all results and unanimously approved the final version of the manuscript.
AVAILABILITY OF DATA AND MATERIALS
The data and supportive information are available within the article.
ACKNOWLEDGEMENTS
The authors wish to thank the Gram Positive Laboratory, Tamil Nadu, India, for their assistance in microbiological laboratory work.

