All published articles of this journal are available on ScienceDirect.

Risk Factors for Caries in Children and Adolescents: A Systematic Review
Authors Info & Affiliations
Abstract
Introduction
Tooth decay is a bacterial infection influenced by a multifactorial interplay of risk factors. This review aimed to examine both established and emerging determinants of dental caries in children and adolescents, with an emphasis on dietary and behavioral influences.
Methods
Following PRISMA guidelines and PICOS criteria, a systematic search was performed across PubMed, Scopus, Web of Science, Embase, ClinicalTrials.gov, and Google Scholar for studies published between January 2015 and December 2024. Eligible studies included cross-sectional, cohort, and case-control designs reporting on caries risk factors.
Results
A total of 18 studies met the inclusion criteria. Established risk factors included poor socioeconomic status, high sugar intake, infrequent toothbrushing, younger maternal age, and higher maternal DMFT scores. Emerging risk factors were nighttime feeding, prolonged breastfeeding beyond 18 months, lack of parental supervision during toothbrushing, maternal unemployment, and single motherhood. Additional associations included low birth weight, poor dietary diversity, and inadequate fluoride exposure.
Discussion
The findings highlight the multifactorial and context-specific nature of caries development in young populations. While traditional risk factors remain highly relevant, newer determinants such as feeding practices and parental factors require further validation through longitudinal and interventional research. Variability in diagnostic tools and methodological heterogeneity across studies limits direct comparability.
Conclusion
This review underscores both established and emerging risk factors for childhood caries. Identifying these determinants may guide preventive strategies, particularly for vulnerable populations, and may inform policy and clinical interventions.
1. INTRODUCTION
Tooth decay is a bacterial infection that results in localized destruction of dental hard tissues, caused by acidic by-products produced during the bacterial fermentation of dietary carbohydrates. Multiple risk factors, including high sugar consumption, poor oral hygiene, socioeconomic status, urbanization rates, and maternal education levels, influence this disease. However, tooth decay is preventable, and early intervention can halt its progression. Regular dental check-ups, proper oral hygiene practices, and a balanced diet are essential for preventing tooth decay and maintaining overall oral health. Effective management requires a comprehensive approach that considers the multifactorial nature of the disease [1].
The primary causes of tooth decay remain unchanged, with susceptible tooth surfaces, Streptococcus mutans, and fermentable carbohydrates recognized as key etiological agents. As a multifaceted disease, understanding these risk factors is essential for developing effective prevention strategies, reducing its prevalence, and identifying at-risk populations. By acknowledging these complexities, dental professionals can tailor interventions to mitigate caries risk and promote optimal oral health outcomes [2, 3].
Young children are particularly vulnerable to tooth decay due to distinct factors affecting their developing oral environment. The maturation of their oral microbial flora and defense mechanisms makes them more susceptible to cariogenic bacterial colonization. Newly erupted primary teeth often have hypoplastic defects or structural weaknesses, increasing their risk of decay. Additionally, the dietary transition from breastfeeding or bottle feeding to solid foods introduces new caries risks, especially with frequent exposure to sugary or starchy foods and beverages [2].
Parental awareness and education are crucial in preventing tooth decay in young children. Caregivers should be informed about proper oral hygiene practices, the importance of limiting sugary and starchy foods, and the need for regular dental visits. Preventive measures such as fluoride varnishes and sealants can further protect children's teeth. Adolescence is also a critical period for establishing lifelong oral health habits [4, 5].
Although several systematic reviews have examined traditional risk factors for dental caries in children, such as sugar consumption, poor oral hygiene, and lack of fluoride exposure, these reviews often focus on high-income settings and overlook emerging determinants like nighttime bottle feeding, maternal employment, health system access, and sociocultural influences common in low- and middle-income countries. Furthermore, existing reviews typically lack a focus on integrating both clinical and public health perspectives in a global context. This review aims to fill that gap by synthesizing evidence across diverse regions and including both well-established and novel caries risk factors in paediatric populations.
Given the significance of these factors, this systematic review aimed to:
- Identify and summarize established risk factors for dental caries in children and adolescents (e.g., sugar intake, oral hygiene, fluoride exposure).
- Highlight and assess emerging or context-specific determinants, including maternal, behavioral, and environmental factors.
- Explore regional and socioeconomic variations in caries risk profiles, with emphasis on low- and middle-income countries.
- Evaluate the quality and consistency of the evidence across diverse study designs and populations.
2. MATERIALS AND METHODS
The review is registered in the PROSPERO database (International Prospective Register of Systematic Reviews) with the reference ID CRD42025632197.
The inclusion criteria were organized following the internationally accepted PICOS framework, in accordance with PRISMA guideline recommendations:
2.3. Comparators/control
Studies were considered for inclusion regardless of whether they incorporated a comparator group.
2.4. Outcome
The primary outcomes assessed were factors associated with and not linked to tooth decay.
2.5. Study Design
All types of experimental studies, observational studies, and case series that reported procedures and outcomes related to the contributing factors of tooth decay were included.
2.6. Eligibility Criteria
2.6.1. Inclusion Criteria
- Peer-reviewed original studies published in English between January 2015 and December 2024.
- Cross-sectional, cohort, or case-control studies reporting on risk factors for dental caries in children and adolescents.
- Studies with clearly defined outcomes related to dental caries (e.g., decayed, missing, and filled teeth (DMFT), International Caries Detection and Assessment System (ICDAS), or WHO criteria).
- Studies providing sufficient methodological details to assess quality and risk of bias.
2.7. Literature Search
A comprehensive literature search was conducted using the following major databases: PubMed, Scopus, Web of Science, and Embase. These databases were selected due to their wide acceptance in systematic reviews and their comprehensive indexing of peer-reviewed biomedical and dental research. In addition, ClinicalTrials.gov and Google Scholar were searched to identify relevant gray literature and ongoing or unpublished studies. The use of multiple databases ensured a broad and inclusive search strategy that minimized publication bias.
2.8. Screening and Selection Process
The search strategy for this review consisted of three sequential stages: screening titles, reviewing abstracts, and selecting articles for full-text analysis. Two independent reviewers (the first and second authors) conducted the initial sorting of articles identified through the database search. Any discrepancies in selection were resolved through discussion until consensus was achieved. Articles failing to meet the predefined inclusion criteria were excluded following agreement between the reviewers. Subsequently, the same reviewers independently assessed the abstracts of articles that passed the second stage, and full texts were obtained for those selected for final analysis.
All citations, along with titles and abstracts, were imported into a dedicated EndNote library, where duplicates were identified and removed to prepare the final list of studies. Full-text articles of all shortlisted studies were then retrieved and evaluated for eligibility. The entire screening and selection process was systematically documented using the PRISMA flowchart to ensure transparency and reproducibility (Fig. 1).
2.9. Data Extraction
The data from the selected studies were thoroughly examined and systematically extracted into a predefined data collection form. Information related to various risk factors for tooth decay was systematically collected and documented.
2.10. Data Synthesis and Analysis
Due to the heterogeneity of the included studies in terms of design, populations, diagnostic criteria (e.g., ICDAS, DMFT, WHO), outcomes, and risk factors evaluated, a meta-analysis was not feasible. Instead, a narrative synthesis approach was adopted.
The studies were grouped and compared according to geographic location, population characteristics, study objectives, and the nature of caries risk factors reported (e.g., dietary, behavioral, socioeconomic, biological). Key themes, consistencies, and divergences in findings were systematically summarized.
Measures of effect, such as odds ratios, prevalence rates, or relative risks, were extracted where available; however, they were not pooled quantitatively due to variability in statistical reporting and methodological frameworks.
2.11. Risk of Bias in Individual Studies
The risk of bias for all included studies was assessed using the Fowkes and Fulton critical appraisal checklist, which evaluates domains such as sample representativeness, control of confounders, validity of outcome measurement, and statistical analysis [6]. Based on the responses, each study was categorized as low, moderate, or high risk of bias.
3. RESULTS
3.1. Study Characteristics
Table 1 provides a summary of 18 studies conducted worldwide between 2015 and 2024. These studies examined various aspects of tooth decay in children, including prevalence, risk factors, and preventive strategies. The studies employed diverse research designs, such as cross-sectional surveys, cohort studies, and retrospective analyses. Where study duration or participant numbers were not available in the original article, these are marked as ‘Not Reported’ for transparency.
3.1.1. Countries and Regions
The studies were conducted across diverse countries, including India, Ethiopia, Thailand, Uganda, the Philippines, the United States, Saudi Arabia, the United Kingdom, Australia, Hong Kong, Iran, and Denmark. This geographical diversity provides a comprehensive understanding of tooth decay in children across different cultural and socioeconomic contexts.
3.2. Research Designs and Methods
A variety of research designs were employed, including cross-sectional surveys, cohort studies, and retrospective analyses. Some studies incorporated mixed-methods approaches, integrating both qualitative and quantitative data collection and analysis. Various assessment tools and criteria were used to diagnose tooth decay, including the DMFT, ICDAS, and WHO.
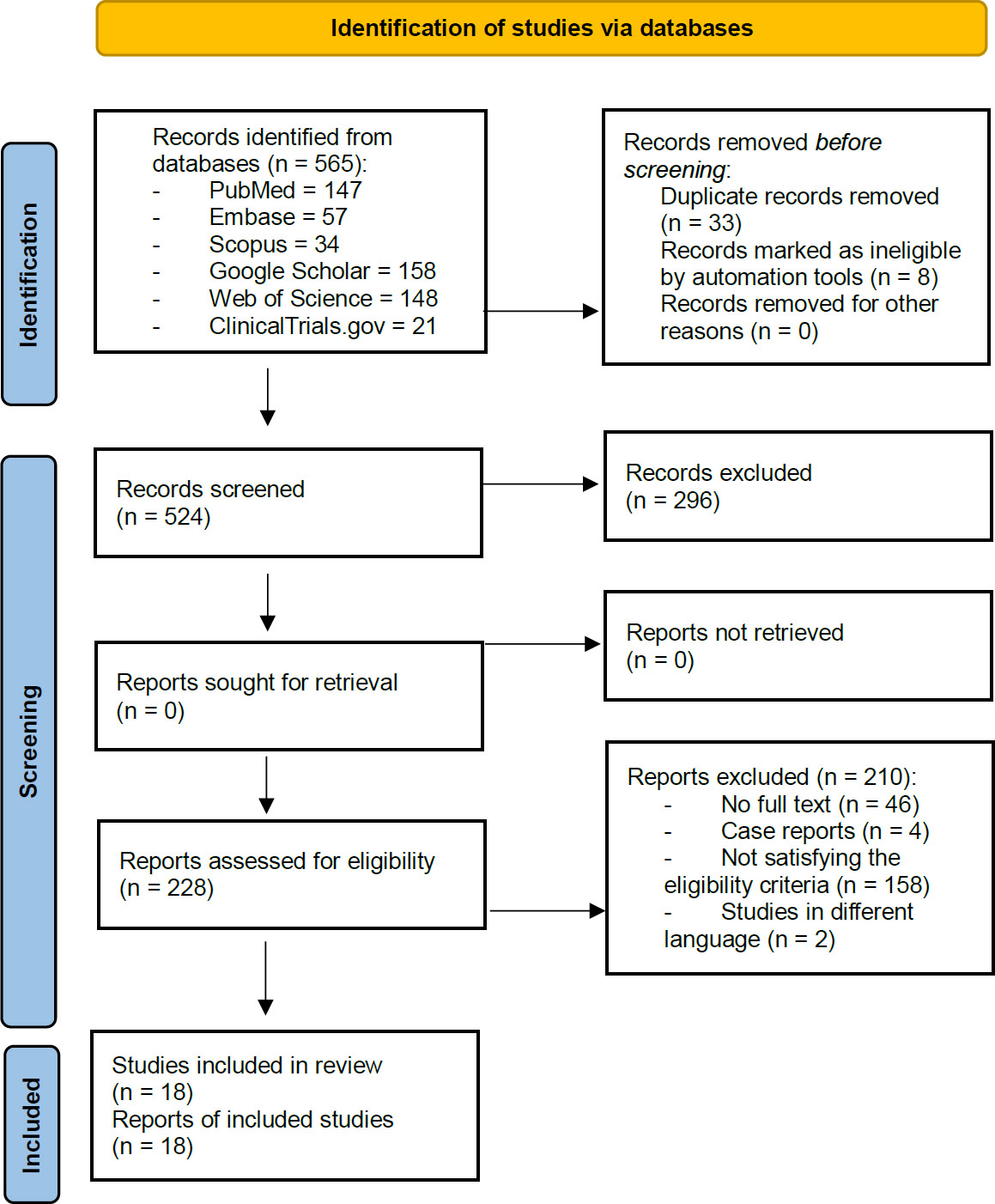
PRISMA 2020 flow diagram showing study selection process.
Note: The Flow chart summarizes the screening and inclusion process for the systematic review.
Source: PRISMA 2020.
Table 1.
| S. No. | Author | Year | Country | Type of Study | Duration of Study | Total Number of Participants | Age Group |
|---|---|---|---|---|---|---|---|
| 1. | Ndagire et al. [5] | 2020 | Uganda | Cross-sectional survey | Not reported | 406 | 11-19 years |
| 2. | Mohanty et al. [7] | 2024 | India | Mixed-method (qualitative + quantitative) |
Not reported | 419 | 6-14 years |
| 3. | Adugna et al. [8] | 2024 | Ethiopia | School-based cross-sectional study | 3 months | 354 | 36-71 months |
| 4. | Tesfay et al. [9] | 2024 | Ethiopia | Cross-sectional study | 4 months | 380 children | 12–36 months |
| 5. | Sritangsiriku et al. [10] | 2024 | Thailand | Cohort study | 2 years | 486 toddlers | Toddler (1-3 years) |
| 6. | Oliveros-Villarico et al. [11] | 2024 | Philippines | Cross-sectional study | Not reported | 703 | 4-24 months |
| 7. | Reddy et al. [12] | 2020 | India | Cross-sectional survey | 1 year | 200 | 13–17 years |
| 8. | Chugh et al. [13] | 2018 | India | Community-based cross-sectional | Not reported | 425 | 3-6 years |
| 9. | Ruff et al. [14] | 2018 | United States of America | Retrospective analysis of a 6-year prospective cohort | Not reported | Not reported | School-going children |
| 10. | Alhabdan et al. [15] | 2018 | Saudi Arabia | Cross-sectional study | 3 months | 578 | 6-8 years |
| 11. | Mangla et al. [16] | 2017 | India | Cross-sectional study | Not reported | 510 | 12-36 months |
| 12. | Bernabé et al. [17] | 2017 | United Kingdom | Longitudinal caries-risk assessment | 4 years | 1,102 | 1-4 years |
| 13. | Arora et al. [18] | 2017 | Australia | Cross-sectional survey | Not reported | 495 | 5–10 years |
| 14. | Chen et al. [19] | 2017 | Hong Kong | Cross-sectional survey | Not reported | 501 | 5 years |
| 15. | Nirunsittirat et al. [20] | 2016 | Thailand | Cohort study | Not reported | 556 | The second trimester of pregnancy to 36 months |
| 16. | Almasi et al. [21] | 2016 | Iran | Cross-sectional survey | 4 months | 698 | 10-12 years |
| 17. | Warren et al. [22] | 2016 | United States of America | Cross-sectional survey | Not reported | 232 | 4, 8, 12, 16, 22, 28, and 36 months of age |
| 18. | Lempert et al. [23] | 2015 | Denmark | Follow-up study | Not reported | Not reported | 9 and 15 years |
Table 2 provides a detailed summary of 18 studies conducted globally between 2015 and 2024, highlighting the risk factors associated with tooth decay in children, along with the research designs, assessment parameters, and analysis methods employed.
| S. No. | Author | Assessment Parameters | Associated Factors | Non-associated Factors |
|---|---|---|---|---|
| 1. | Ndagire et al. [5] | DMFT index: a questionnaire |
- Tooth cleaning device used - Child's age - History of previous dental visits |
Not mentioned |
| 2. | Mohanty et al. [7] | DMFT/DEFT index; For qualitative analysis, Parents and teachers were interviewed about children's dietary habits, dental hygiene, and tobacco chewing behaviors |
- Age, poor socioeconomic status, and high frequency of sugar and chocolate consumption | Not mentioned |
| 3. | Adugna et al. [8] | Questionnaire with sociodemographic-related characteristics, as well as dietary and oral hygiene-related characteristics | - Nighttime feeding (AOR=3.98) - Lack of parental supervision during toothbrushing (AOR=2.98) - Previous dental visits (AOR=3.05) |
Being overweight or obese (actually found to be protective, AOR=0.29) |
| 4. | Tesfay et al. [9] | WHO Dental Caries Measure: Decayed-Extracted-Filled Teeth Exposure Variable: Breastfeeding duration refers to the overall length of time that any breastfeeding was practiced, Structured questionnaires |
- Sugar consumption: ≥ 2 times/day increases caries risk by 2.34 times (OR = 2.34, 95% CI: 1.27-4.31) - Child age: 24-36 months old increases caries risk by 2.44 times (OR = 2.44, 95% CI: 1.42-4.22) compared to 12-23 months old - Mother's employment: Unemployed mothers increase caries risk by 1.95 times (OR = 1.95, 95% CI: 1.05-3.61) - Mother's marital status: Single mothers increase caries risk by 2.77 times (OR = 2.77, 95% CI: 1.58-4.86) |
Breastfeeding duration showed no significant association with dental caries |
| 5. | Sritangsirikul et al. [10] | Decayed-and-filled-teeth, Full breastfeeding |
- Full breastfeeding for a moderate duration (6–17 months) provides protective effects, whereas breastfeeding for 18 months or longer is associated with an increased risk in this population | - |
| 6. | Oliveros-Villarico et al. [11] | Caregivers were interviewed, and dental exams were conducted by a calibrated dentist using the ICDAS for each child | 4. Child's age 5. Caregiver's low educational level 6. Continued breastfeeding 7. Frequent eating (6 times/day) 8. Visible plaque on teeth (observed by caregiver and in oral examination) |
Not mentioned |
| 7. | Reddy et al. [12] | Questionnaire, Silness and Löe plaque index, ICDAS-II 22 |
- A reduced pH level was found to be statistically significant in cases of moderate and extensive caries, respectively - Saliva quantity showed a statistically significant association with mild and moderate caries - A low buffering capacity was linked to the presence of mild caries |
Not mentioned |
| 8. | Chugh et al. [13] | Questionnaire: dental caries was diagnosed as per the WHO guidelines 2013 | - Longer duration of breastfeeding (>36 months, 12-24 months) - Increase in age (61-72 months, 49-60 months) - Having more than two children in the family - Lack of parental supervision during toothbrushing |
Gender of the children, caste, and religion |
| 9. | Ruff et al. [14] | Retrospective analysis | - Within both school and community settings, residing in a dental-shortage area and a higher proportion of children receiving free or reduced lunch were significantly associated with an increased baseline risk of dental caries | Not mentioned |
| 10. | Alhabdan et al. [15] | Questionnaire | 1. Socioeconomic factors: - Limited maternal education - Low household income - Absence of dental insurance (associated with a ≥ 4-fold increase in risk) 2. 2. Oral hygiene habits: - Infrequent brushing (< 1/day) - Delayed brushing onset (> 2 years) - Symptomatic dental visits 3. Feeding habits: - Sleeping with a bottle in the mouth (4.4-fold increased risk) - Lack of mixed feeding - Consuming ≥ 2 sugary snacks between meals 4. Dietary habits: - Inadequate intake of fresh fruits - Frequent consumption of soft drinks and flavored milk |
Not mentioned |
| 11. | Mangla et al. [16] | Caries was recorded using the WHO criteria; Questionnaire | - Child's age group - Mother's educational level - Length of time the child used a bottle - Level of adult supervision during toothbrushing - Frequency of consuming sugary and sticky foods |
Mother working or nonworking, Income, Father’s education level, Age of commencement of solids |
| 12. | Bernabé et al. [17] | Assessment of caries (dmfs) at 1 y (baseline), repeated annually from ages 1 to 4 |
- Low birth weight (with increased rate of change in dmfs) - Maternal smoking (with increased rate of change in dmfs) |
Breastfeeding duration (with childhood caries) |
| 13. | Arora et al. [18] | The questionnaire included sections on socio-demographic details, oral hygiene practices, dietary habits, residential mobility, and dental visitation history | - Child's Age: Every additional year increases caries odds by 30% (OR = 1.30, 95% CI: 1.14-1.49) - Chocolate Consumption: Each additional serve increases caries odds by 52% (OR = 1.52, 95% CI: 1.19-1.93) - Mother's Extraction History: Every tooth extracted increases the child's caries odds by 2 times (OR = 2.05, 95% CI: 1.40-3.00) |
Not mentioned |
| 13. | Arora et al. [18] | The questionnaire included sections on socio-demographic details, oral hygiene practices, dietary habits, residential mobility, and dental visitation history | - Other significant factors: - Frequency of toothbrushing - Age at which toothbrushing was initiated - Type of toothpaste used - History of exposure to fluoridated water - Consumption of sugary beverages - Parental age and educational attainment - Extraction history of both parents - Household income level |
Not mentioned |
| 14. | Chen et al. [19] | Questionnaire survey and a clinical examination (DMFT) | - Frequent sugary snack consumption (≥2 times/day), irregular dental attendance, low parental dental knowledge levels, low maternal education levels (primary education or below), low family income, and a grandparent as primary caregiver | Gender (boys vs. girls), Birthplace |
| 15. | Nirunsittirat et al. [20] | A structured questionnaire was used to interview mothers or caregivers during the second trimester of pregnancy and at multiple time points postnatally: 21 days, and at 3, 12, 18, 24, and 36 months after birth | - Sleeping while feeding, full breastfeeding (6-11 months), with lower DMFS and a lower caries prevalence | Prolonged breastfeeding or breastfeeding duration |
| 16. | Almasi et al. [21] | Structured questionnaire | - Female gender (increased odds of caries susceptibility) - Frequent consumption of: - Fizzy soft beverages (>1/day) - Sweet biscuits (>1/day) |
Not mentioned |
| 17. | Warren et al. [22] | Dental exams and maternal questionnaires were administered at baseline and at 4, 8, 12, 16, 22, 28, and 36 months | - Increased consumption of beverages with added sugars - Younger maternal age - Elevated maternal DMFT scores - Larger household size |
Not mentioned |
| 18. | Lempert et al. [23] | DMFT | - Dairy and milk consumption, as well as their components like calcium, whey, and casein, were found to be inversely related to childhood and adolescent caries experience | Not mentioned |
3.3. Associated Risk Factors
The studies identified several risk factors (Table 3) significantly linked to tooth decay in children, including:
3.3.1. Socioeconomic Factors
Low maternal education, limited family income, and absence of dental insurance.
3.3.2. Dietary Habits
Frequent consumption of sugary snacks and drinks, bedtime bottle-feeding habit, and low intake of fresh fruits.
3.4. Non-associated Risk Factors
Some studies found no significant association between tooth decay and the following factors:
1 Breastfeeding duration.
2 Gender.
3 Birthplace.
4 Mother's working status, income, and father's education level.
3.5. Established Risk Factors
The following are well-documented risk factors for tooth decay in children:
3.5.1. Poor Socioeconomic Status
Low family income, low maternal education, and lack of dental insurance increase caries risk.
3.5.2. High Sugar Consumption
Frequent intake of sugary snacks and drinks, including fizzy soft beverages and sweet biscuits, significantly increases caries susceptibility.
3.5.3. Poor Oral Hygiene Habits
Infrequent brushing and delayed onset of brushing contribute to increased caries risk.
3.5.5. Higher Maternal DMFT
A greater number of DMFT in mothers is linked to increased caries risk in their children.
| Category | Risk Factor | Description | References |
|---|---|---|---|
| Established Risk Factors | Poor socioeconomic status | Consistently associated with dental caries | Mohanty et al., 2024 [7]; Alhabdan et al., 2018 [15] |
| High frequency of sugar consumption | Strongly linked to dental caries in several studies | Tesfay et al., 2024 [9]; Chen et al., 2017 [19] | |
| Infrequent brushing | Recognized as a potential risk factor for tooth decay | Alhabdan et al., 2018 [15]; Chugh et al., 2018 [3] | |
| Consuming sugary snacks and drinks | Recognized as a potential risk factor for tooth decay | Tesfay et al., 2024 [9]; Chen et al., 2017 [19] | |
| Prolonged breastfeeding | Recognized as a potential risk factor for tooth decay | Sritangsirikul et al., 2024 [10]; Chugh et al., 2018 [13] | |
| Emerging Risk Factors | Mother’s employment status | Unemployed mothers found to have increased caries risk | Tesfay et al., 2024 [9] |
| Lack of parental supervision during toothbrushing | Recognized as a potential risk factor for tooth decay | Adugna et al., 2024 [8]; Chugh et al., 2018 [13] | |
| Previous dental visits | Found to be a risk factor for dental caries in some studies | Adugna et al., 2024 [8]; Warren et al., 2016 [22] | |
| Mother’s marital status | Single mothers found to have increased caries risk | Tesfay et al., 2024 [19] | |
| Low maternal education | Recognized as a potential risk factor for tooth decay | Alhabdan et al., 2018 [15]; Chen et al., 2017 [19] |
3.6. Emerging Risk Factors
Recent studies have identified additional factors that may contribute to tooth decay in children:
3.6.2. Prolonged Breastfeeding
Breastfeeding beyond 18 months may elevate the risk of caries development.
3.6.3. Lack of Parental Supervision during Toothbrushing
Children without proper supervision during oral hygiene routines face a higher risk of caries.
3.6.4. Mother's Employment Status
Unemployed mothers may be linked to a greater risk of tooth decay in children.
3.7. Risk of Bias Assessment
As shown in Table 4, the majority of included studies were assessed as having low to moderate risk of bias, with only two studies classified as high risk due to insufficient control for confounding variables or incomplete data reporting.
4. DISCUSSION
Tooth decay is a prevalent global oral health issue affecting individuals of all ages, with children being particularly vulnerable [24]. This study aimed to identify both established and emerging risk factors for tooth decay by analyzing research conducted over the past decade. Established risk factors include poor socioeconomic status, high sugar consumption, poor oral hygiene habits, younger maternal age, and higher maternal DMFT scores. Specifically, low family income, low maternal education, and lack of dental insurance were consistently linked to increased caries risk. Additionally, frequent consumption of sugary foods, infrequent brushing, and delayed initiation of oral hygiene practices were also major contributors.
Emerging risk factors, such as nighttime feeding, prolonged breastfeeding beyond 18 months, lack of parental supervision during toothbrushing, unemployment among mothers, single motherhood, and low birth weight, were also identified. These factors may further increase children's susceptibility to tooth decay. Recognizing both established and emerging risk factors is crucial for developing.
This systematic analysis encompassed studies employing diverse research designs, including cross-sectional surveys, cohort studies, and retrospective analyses. Several studies employed mixed-methods approaches, combining qualitative and quantitative data collection and analysis. The included studies employed various diagnostic criteria for assessing dental caries, including ICDAS, the WHO, and the DMFT index, as well as other region-specific classification methods. While each tool has its own merits, such variability may introduce inconsistencies in outcome measurement, severity classification, and disease thresholds. To address this, findings were synthesized qualitatively and grouped based on the general presence or absence of disease, rather than strictly comparing caries severity scores across systems. This approach allowed for thematic consistency despite methodological differences. Nevertheless, the use of different diagnostic tools remains a limitation in terms of cross-study comparability and generalizability [25-30].
| Study | Sample Representativeness | Control for Confounders | Outcome Measurement | Statistical Validity | Overall Risk of Bias |
|---|---|---|---|---|---|
| Ndagire et al. [5] | Low Risk | Low Risk | Low Risk | Low Risk | Low |
| Mohanty et al. [7] | Low Risk | Moderate Risk | Low Risk | Low Risk | Moderate |
| Adugna et al. [8] | Low Risk | Low Risk | Low Risk | Low Risk | Low |
| Tesfay et al. [9] | Low Risk | Low Risk | Low Risk | Low Risk | Low |
| Sritangsirikul et al. [10] | Low Risk | Low Risk | Low Risk | Low Risk | Low |
| Oliveros-Villarico et al. [11] | Low Risk | Low Risk | Moderate Risk | Moderate Risk | Moderate |
| Reddy et al. [12] | Low Risk | Moderate Risk | Low Risk | Low Risk | Moderate |
| Chugh et al. [13] | Moderate Risk | Moderate Risk | Moderate Risk | Moderate Risk | Moderate |
| Ruff et al. [14] | Moderate Risk | High Risk | Moderate Risk | Moderate Risk | High |
| Alhabdan et al. [15] | Low Risk | Low Risk | Low Risk | Low Risk | Low |
| Mangla et al. [16] | Low Risk | Moderate Risk | Moderate Risk | Low Risk | Moderate |
| Bernabé et al. [17] | Low Risk | Low Risk | Low Risk | Low Risk | Low |
| Arora et al. [18] | Low Risk | Moderate Risk | Moderate Risk | Low Risk | Moderate |
| Chen et al. [19] | Low Risk | Moderate Risk | Moderate Risk | Moderate Risk | Moderate |
| Nirunsittirat et al. [20] | Low Risk | Moderate Risk | Low Risk | Low Risk | Moderate |
| Almasi et al. [21] | Low Risk | Low Risk | Low Risk | Low Risk | Low |
| Warren et al. [22] | Low Risk | Moderate Risk | Low Risk | Moderate Risk | Moderate |
| Lempert et al. [23] | Moderate Risk | Not Reported | Moderate Risk | Moderate Risk | Moderate |
This analysis identified multiple contributing factors significantly associated with tooth decay in children, including socioeconomic elements such as low maternal education, limited family income, and absence of dental insurance. Additionally, dietary habits such as frequent consumption of sugary snacks and beverages, nighttime bottle-feeding, and low intake of fresh fruits were also associated with tooth decay. Oral hygiene habits, including infrequent brushing, delayed onset of brushing, and lack of parental supervision during toothbrushing, were also identified as risk factors. Demographic factors like a child's age, gender, and birth weight, as well as parental factors such as maternal smoking, younger maternal age, and higher maternal DMFT, were also linked to tooth decay. Some studies found no significant association between tooth decay and certain factors. These non-associated risk factors include breastfeeding duration, gender, birthplace, mother's working status, income, and father's education level. These findings indicate that these factors might not have a significant impact on the development of tooth decay in children. Our findings align with existing literature. A meta-analysis of case-control studies by Shrestha et al. reported that shorter breastfeeding durations were associated with fewer instances of tooth decay. Specifically, children breastfed for less than six months exhibited significantly fewer caries (OR = 0.53, p < 0.001) compared to those breastfed for six months or more [31]. Similar trends were observed for breastfeeding durations of less than 12 months (RR = 0.65, p = 0.002) and less than 18 months (RR = 0.41, p = 0.030). However, nocturnal breastfeeding was found to increase the risk of Early Childhood Caries (ECC) by 2.35 times (RR = 2.35, p < 0.001). A review by Thang Le et al. identified additional potential risk factors for ECC, such as enamel defects, elevated levels of mutans streptococci, existing dentinal caries, soda consumption, daily sugary snack intake, and obesity [32]. Likewise, a systematic review conducted by Tham et al. reported that breastfeeding duration had a variable impact on caries risk. While children breastfed up to 12 months had a lower risk (OR 0.50; 95% CI: 0.25–0.99), breastfeeding beyond 12 months was linked to a greater tooth decay (OR 1.99; 95% CI: 1.35–2.95). Additionally, nocturnal or frequent breastfeeding beyond 12 months was linked to an even greater caries risk [33].
A study by Arora et al. identified key risk factors for primary dentition caries, highlighting three significant contributors. Firstly, each additional year of a child’s age increased their odds of developing caries by 30% (OR = 1.30, 95% CI: 1.14-1.49). Secondly, each additional serving of chocolate was associated with a 52% (OR = 1.52, 95% CI: 1.19-1.93) increase in the likelihood of the child developing dental caries. Thirdly, each tooth extracted from the mother’s mouth doubled the child’s caries risk (OR = 2.05, 95% CI: 1.40-3.00). Other significant factors identified through univariate analysis included toothbrushing frequency, age at brushing initiation, type of toothpaste used, prior exposure to fluoridated water, consumption of sugary beverages, parental education level, extraction history of both parents, and household income [18]. Similarly, a study by Warren et al. using logistic regression analysis identified significant risk factors for tooth decay, including higher consumption of added-sugar beverages, younger maternal age, higher baseline maternal DMFT scores, and larger household size. Negative binomial regression analysis revealed a strong association between maternal DMFT scores and children's DMFT counts, underscoring the significant impact of maternal oral health on the risk of dental caries in children [22].
Unsupervised toothbrushing was linked to a higher risk of Severe Early Childhood Caries (S-ECC), with affected children more likely to brush independently without adult assistance. This finding aligns with prior research by Mahejabeen et al. [34]. S-ECC is a common condition characterized by the presence of decayed, missing, or filled surfaces in the primary teeth of children younger than 71 months [34]. If not addressed promptly, S-ECC can substantially diminish a child's quality of life, while also increasing the complexity of treatment and associated healthcare costs [34]. One of the strongest predictors of S-ECC was prolonged bottle-feeding, with bottle-fed children demonstrating a significantly higher risk than those who transitioned to regular cups earlier. Multiple regression analysis confirmed this association [16]. To mitigate the risk of S-ECC, caregivers should be educated on appropriate feeding practices, including avoiding on-demand breastfeeding, discouraging prolonged bottle use, transitioning to a cup by 12 months, and regular mouth cleaning after tooth eruption. Additionally, frequent consumption of sweet and sticky snacks was strongly correlated with an increased risk of S-ECC, a finding supported by multiple studies [35-37].
A study by Cascaes et al. found that consuming large amounts of ultra-processed foods was linked to a higher risk of tooth decay in young individuals [38]. According to the NOVA Food Classification System, ultra-processed foods are industrially manufactured products composed of extracted food substances, such as oils, sugars, and starches, and typically contain added synthetic flavors, colors, and preservatives to improve taste and appeal [38].
The U.S. Centers for Disease Control and Prevention acknowledges water fluoridation as one of the most significant public health achievements of the 20th century, owing to its effectiveness in reducing oral health disparities [39]. Consistent research findings indicate that water fluoridation leads to a 15.4% increase in the proportion of children free from tooth decay [40]. Multiple studies have emphasized the protective benefits of water fluoridation, revealing that individuals in non-fluoridated communities bear a significantly greater burden of tooth decay compared to those residing in areas with fluoridated water [41, 42]. A 2024 meta-analysis by Iheozor-Ejiofor et al. reviewed 107 studies and confirmed that water fluoridation significantly reduces tooth decay. Specifically, fluoridation resulted in a 35% reduction in decay of deciduous teeth and a 26% reduction in decay of permanent teeth. Furthermore, water fluoridation increased the proportion of caries-free children by 15% in deciduous teeth and 14% in permanent teeth. However, approximately 12% of participants developed dental fluorosis with aesthetic concerns at a fluoride concentration of 0.7 ppm [40].
Earlier, Parisotto et al. reported a greater caries burden in children residing in non-fluoridated areas compared to those living in fluoridated regions [43]. A large-scale study by Do et al. revealed a 40% lower caries occurrence rate among children in long-term fluoridated areas compared to those in non-fluoridated areas [41]. Similarly, Lee et al. observed a significant rise in caries prevalence among children aged 5–6 and 11–12 years living in low-fluoridated or non-fluoridated areas compared to those residing in fluoridated regions [44]. Pierce et al. investigated multiple factors influencing Early Childhood Caries (ECC), including age, sex, socioeconomic status, parental beliefs, family characteristics, oral hygiene habits, and feeding practices in Canadian children. The study found that ECC was closely linked to social determinants of health, such as lower household income, parental education level, and employment status. Additional risk factors included age at first dental visit, parental attitudes toward oral health, and the presence of enamel hypoplasia, which significantly increased caries risk [45]. Similarly, Guido et al. identified an increased risk of caries associated with the consumption of sugary drinks, inadequate oral hygiene practices, and limited access to fluoridated tap water [3].
An analysis by Branger et al. suggested that breastfeeding for less than one year has a protective effect against childhood caries. However, beyond one year, the impact remains unclear due to confounding factors such as dietary habits and oral hygiene practices. To mitigate potential caries risks, dental consultation is recommended for children breastfed beyond one year, with personalized guidance on diet, oral hygiene, and fluoride supplementation [46]. A study by Do concluded that socioeconomic status and behavioral habits remain the dominant predictors of caries, with emerging variables acting more as modifiers than direct causal agents [47].
In addition to the established risk factors identified, aging and malocclusion also influence caries experience. A study of 748 adolescents by Eslamipour et al. showed that mean DMFT scores increased with age, rising from 3.03 in 11–14-year-olds to 6.66 in 17–20-year-olds, with strong positive correlations between age and DMFT, decayed teeth, and filled teeth scores [48]. Malocclusion, assessed using the Dental Aesthetic Index in the study by Borzabadi-Farahani et al., was associated with higher caries experience, particularly in children from larger households (more than six members), where severe caries prevalence increased with malocclusion severity. In this subgroup, children with orthodontic treatment needs were 4.6 times more likely to have severe caries [49]. These findings emphasize that both aging and malocclusion, especially when compounded by socioeconomic factors, should be considered in comprehensive caries risk assessments. Thus, while these novel findings warrant further investigation, they should not overshadow the importance of prioritizing preventive strategies against well-validated caries determinants.
Several unmeasured or unadjusted confounding factors may have influenced the associations reported in the included studies. For instance, access to dental care, genetic susceptibility to enamel defects, and local public health infrastructure (e.g., water fluoridation, preventive services) can significantly alter caries risk, independent of behavioral factors such as diet or oral hygiene. These confounders were not consistently controlled for across studies, limiting the ability to draw strong causal inferences. Future studies should apply multivariable analysis techniques to adjust for such variables and better isolate the effects of modifiable risk factors.
The findings of this review carry important implications for both public health policy and clinical practice. The consistent association of dental caries with modifiable factors such as sugar intake, poor oral hygiene, parental neglect, and lack of fluoride exposure supports the need for comprehensive school-based oral health programs, community fluoridation, and parental education initiatives. For clinical application, the results reinforce the value of early caries risk assessment, especially in children with high-risk socioeconomic backgrounds or those exhibiting poor oral habits. Pedodontics and primary care providers should be trained to incorporate these risk indicators into routine examinations.
5. LIMITATIONS
This review has several limitations. First, we only included peer-reviewed, published studies, which means that some relevant but unpublished or non-traditional research, such as theses or reports found in gray literature, might have been missed. Although we searched broad platforms like Google Scholar, we did not use specific gray literature databases such as OpenGrey or ProQuest, which could have introduced some selection bias. Second, the studies we included varied widely in terms of design, participant characteristics, how they measured outcomes, and which diagnostic tools they used (like ICDAS, DMFT, or WHO criteria). This made it difficult to compare results across studies and may have affected the consistency of our findings.
Additionally, not all studies reported the duration of their experiments, which made it more challenging to assess the reliability of their results over time. Third, since we only reviewed studies published in English, we may have missed valuable data from non-English-speaking countries. Lastly, because the included studies used different methods and did not consistently report statistical measures, we were not able to perform a meta-analysis. Instead, we relied on a narrative summary, which limits the precision with which we can measure the strength of the reported associations.
CONCLUSION
This systematic review highlights that dental caries in children and adolescents is consistently associated with modifiable factors such as frequent sugar consumption, poor oral hygiene, inadequate fluoride exposure, and low parental education. While emerging factors such as nighttime feeding and maternal employment appear relevant in certain contexts, the strength of the evidence remains limited, and further high-quality research is needed to validate these associations. Public health interventions should continue to prioritize established risk factors, particularly in underserved populations, to maximize the effectiveness of these efforts. Future studies should aim for methodological consistency and control for confounding factors to strengthen the evidence base.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contribution to the paper as follows: R.I., S.A.F.A.: Study conception and design; D.A.A.A.: Data collection; S.R.A., R.A.S.A.: Analysis and interpretation of results; L.H.S.A.: Draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| DMFT | = Decayed, Missing, and Filled Teeth |
| ICDAS | = International Caries Detection and Assessment System |
| PRISMA | = Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| PROSPERO | = International Prospective Register of Systematic Reviews |
| ECC | = Early Childhood Caries |
| S-ECC | = Severe Early Childhood Caries |
AVAILABILITY OF DATA OF MATERIALS
The data supporting the findings of the article will be available from the corresponding author [R.I] upon reasonable request.
ACKNOWLEDGEMENTS
Declared none.

