All published articles of this journal are available on ScienceDirect.

Physiological Maturation Indicators as Determinants of Pubertal Growth in Orthodontic Treatment: A Scoping Review
Abstract
Introduction
The pubertal growth period is a critical phase for orthodontic treatment, as its evaluation directly influences diagnostic accuracy and treatment outcomes. Pubertal growth evaluation can be conducted by assessing individual physiological maturation. This study aims to conduct a scoping review to map and determine physiological maturation indicators that are highly correlated with pubertal growth.
Methods
A scoping review was conducted using literature searches in Scopus, PubMed, ScienceDirect, and Google Scholar. The articles used in this review are articles published within the period from 2014 to 2024.
Results
A total of 18 articles out of 279 met the inclusion criteria in this scoping review. Fourteen studies assessed pubertal growth using dental maturation indicators, predominantly the Demirjian method. Two studies used biomarkers such as IGF-1 and ALP. One study evaluated skeletal maturation using fractal dimension analysis, and one study assessed sexual maturation based on menarche status. All studies compared the selected indicators to skeletal maturation.
Discussion
Dental maturation indicators were the most frequently investigated and exhibited a high correlation with skeletal maturation, supporting their use as a practical, non-invasive tool for pubertal growth assessment. Biomarkers such as IGF-1 offer a promising non-radiographic alternative, while supporting evidence for fractal dimension analysis and menarche status remains limited.
Conclusion
Dental maturation is the most reliable indicator of pubertal growth due to its strong correlation with skeletal maturation, while evidence for other indicators, such as fractal dimension and menarche, remains limited. Variations in age range and population may affect the generalizability of these findings.
1. INTRODUCTION
The pubertal growth phase plays a crucial role in orthodontic treatment. Predictions of pubertal growth can affect the diagnosis, treatment objectives, planning, and results of orthodontic therapy [1]. Orthodontic treatment is a treatment that is carried out using orthodontic tools by applying light pressure to the teeth so that they move in a certain direction [2]. Orthodontic treatment can be divided into three types based on the nature and timing of the intervention: preventive orthodontics, interceptive orthodontics, and corrective orthodontics [3]. Interceptive orthodontic treatment is carried out during the growth period or the mixed dentition phase [4]. In orthodontics, the individual growth period represents a critical phase for preventing the progression of severe malocclusions and for modifying maxillomandibular growth discrepancies [1]. The individual growth period consists of accelerated growth followed by a period of slower growth [5]. The period of accelerated growth occurs during puberty [6, 7]. Orthodontists closely monitor periods of accelerated growth, as they can achieve the best growth modification in orthodontic treatment during this time [8]. Once this phase has passed and skeletal growth is complete, orthognathic procedures may be considered, and diagnostic evaluations such as the IOFTN index, ANB angle, and overjet measurements should be performed after growth cessation to ensure accurate assessment and appropriate treatment planning [9, 10]. Therefore, precise identification of the growth period is essential to optimize the timing of orthodontic intervention and to maximize treatment outcomes.
Growth refers to the progressive increase in a child's physical dimensions, including size, height, weight, and length, and is a process that eventually ceases upon reaching physical maturity [11]. Puberty is defined as a period characterized by the emergence of various changes, many of which occur simultaneously, including accelerated growth, changes in body proportions, and the development of secondary sexual characteristics. The amount of growth during puberty is influenced by genetic, endocrine, nutritional, and ethnic factors [12]. The timing and duration of pubertal growth vary between sexes [13]. Females experience pubertal growth earlier than males. The peak of pubertal growth in females occurs earlier than in males, although males tend to complete their growth period earlier than females [14]. Variations in the onset and extent of pubertal growth, both between sexes and within individuals, underscore the importance of evaluating pubertal growth in patients undergoing orthodontic treatment.
Attempts to predict growth, especially during periods of accelerated growth, can use various methods, including chronological age and physiological age [15]. Chronological age is assessed based on the date, month, and year of an individual’s birth [16]. In some cases, a person's chronological age and biological age do not show similarities. Developmental differences and racial variation are believed to cause this dissimilarity [17]. The variation of each individual, especially during growth acceleration, means that chronological age cannot be considered a reliable indicator for assessing the maturation status of an individual, thus giving birth to the idea of biological or physiological maturity [15]. The maturation status of skeletal, dental, somatic, and sexual systems determines an individual’s physiological age [15]. Skeletal maturation is assessed by the degree of bone hardening that can be seen radiologically and through systemic analysis of factors directly responsible for bone growth and remodeling [15, 18]. Tooth maturation is assessed through the evaluation of tooth formation [19]. Somatic maturation is assessed based on morphological changes in the body over time [20]. Sexual maturation assesses secondary sex characteristics to determine an individual’s maturation status [15]. The variation in the use of physiological maturation indicators provides opportunities for further research on their application in assessing pubertal growth.
A study found that the correlation between the pubertal growth phase and Hand-Wrist Maturation (HWM) stage indicates that HWM can be used to identify an individual’s growth phase [14]. In addition, other research suggests that tooth maturation performs well as a diagnostic tool for assessing maturity status. The use of tooth maturation as a method of assessing pubertal growth is reliable. This method will also utilize resources more efficiently and reduce patient radiation exposure [21]. On the other hand, a study investigated the correlation between biomarkers and the pubertal growth period. The study outcomes indicate that no difference was found in salivary B-ALP levels during the pubertal growth period. Therefore, the effectiveness of B-ALP saliva as an indicator of pubertal growth is questionable [22].
Based on the discussion of previous studies' results, which show various variations in research results regarding physiological maturation indicators for pubertal growth, this study aimed to map and identify maturation indicators with a high correlation in assessing pubertal growth through a scoping review, in order to support orthodontic diagnosis and treatment planning.
2. MATERIALS AND METHODS
This study employs a scoping review as its research design. A scoping review is a systematic analysis that maps the available literature on a topic and identifies concepts, theories, sources of evidence, and gaps in the research [23]. This scoping review consists of six stages: identifying research questions, identifying relevant article sources, selecting and extracting data, mapping data, compiling, summarizing, reporting results, and consulting with competent parties [24].
This study began by identifying research questions using the PCC (Population, Concept, and Context) framework. The PCCs of this study are as follows: 1) Population: adolescent patients in puberty aged 8–20 years [25, 26], 2) Concept: indicators of physiological maturation as determinants of pubertal growth [1], and 3) Context: individual growth during the pubertal period.
The search for relevant articles was carried out on three databases: Scopus, PubMed, ScienceDirect, and the Google Scholar search engine. The inclusion criteria for the research materials were articles that met the following conditions: Articles were published between 2014 and 2024 to ensure that the studies reflect current and relevant findings aligned with recent clinical developments, articles related to the correlation of physiological maturation indicators to pubertal growth, articles with the keywords (“Biological Maturation”) OR (“Physiological Maturation”) OR (“Skeletal Maturation”) OR (“Somatic Maturation”) OR (“Sexual Maturation”) OR (“Dental Maturation”)) OR ((“Maturity Physiology Indicator”) OR (“Biological Maturity”) OR (“Physiological Maturity”) OR (“Skeletal Maturity”) OR (“Somatic Maturity”) OR (“Sexual Maturity”) OR (“Dental Maturity”)) AND (“Pubertal Growth”) in searching for articles, and articles with the research subject being individuals in a normal state without abnormalities and adolescents in puberty aged 8-20 years. Exclusion criteria for this study included articles that only contained abstracts and review articles.
Data extraction was carried out by three observers, two of whom independently conducted the screening to identify studies according to the research objectives. If disagreements arose between the two observers, they were resolved by the third observer. The data extracted from each article include the title, author’s name, year of publication, sample, age of sample, race, country, gender, research method, maturation indicator, comparison, results, and conclusion. The presented data were then analyzed using thematic analysis.
3. RESULTS
The procedure for article search and citation retrieval is illustrated in Fig. (1).
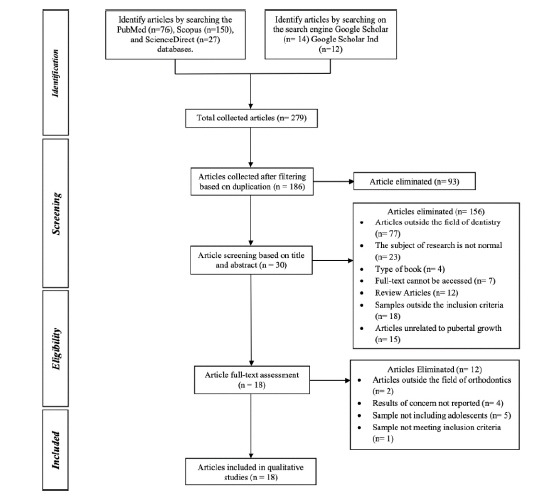
PRISMA-ScR flow chart.
The first stage of the study was to search for articles on three databases and search engines using predefined keywords. The total number of articles collected was 279, with 76 articles on PubMed, 150 on Scopus, 27 on Science Direct, and 26 on Google Scholar. The second stage involved checking for duplicate articles; 186 articles were collected, and 93 articles were eliminated. The next stage was filtering the articles based on the title and abstract; 30 articles were collected, and 156 were eliminated. The remaining 30 articles were examined by reading the full text to assess their feasibility. A total of 12 articles were excluded, resulting in 18 articles for further analysis.
3.1. Literature Characteristics
The literature synthesis was entered into two data tables, consisting of a general data table (Table 1) and a specific data table (Table 2). There were 18 articles obtained, with 14 articles assessing pubertal growth using dental maturation indicators, two articles using skeletal maturation by assessing biomarkers, 1 article using skeletal maturation by assessing fractal dimensions, and 1 article using sexual maturation. All articles compared skeletal maturation indicators to assess their relationship to pubertal growth. Seven articles used cervical vertebrae skeletal maturation as a comparison, six articles used hand-wrist skeletal maturation as a comparison, four articles used cervical vertebrae and hand-wrist skeletal maturation as a comparison, and 1 article used skeletal maturation by assessing the middle segment of the middle finger and dental maturation by the Demirjian method as a comparison.
| No. | Heading | Author (Year) | Sample | Sample Age | Ras | Country | Gender | Research Methods |
|---|---|---|---|---|---|---|---|---|
| 1 | Correlation between skeletal maturation and developmental stages of canines and second molars among iranian population [27] | Firouzinia et al. (2022) | 201 digital panoramic and lateral cephalometric radiographs | 8-15 years | Caucasian | Iran | 89 males and 112 females | Observational study (Cross-sectional study) |
| 2 | Serum and urine insulin-like growth factor-1 as biochemical growth maturity indicators [28] | Sinha et al. (2016) | 72 lateral cephalograms, 5ml blood, and urine | 8-20 years | Asian | India | 72 females | Observational study (Cross-sectional study) |
| 3 | Assessment of correlation between dental calcification stages and skeletal maturity indicators [29] | Ojha et al. (2019) | 50 orthopantomograph (OPG) and hand–wrist radiographs | 8-14 years | Asian | India | 25 males and 25 females | Observational study (Cross-sectional study) |
| 4 | Evaluation of the relationship between the Demirjian and Nolla methods and the pubertal growth spurt stage predicted by skeletal maturation indicators in Turkish children aged 10–15: an investigation study [13] | Günen Yılmaz et al. (2018) | 717 panoramic and hand–wrist radiographs | 10-15 years | Caucasian | Turkey | 334 males and 383 females | Observational study (Cross-sectional study) |
| 5 | Correlation between dental maturity by demirjian method and skeletal maturity by cervical vertebral maturity method using panoramic radiograph and lateral cephalogram [30] | Mini et al. (2018) | 100 panoramic radiographs and lateral cephalograms | 8-16 years | Asian | India | 46 males and 54 females | Observational study (Cross-sectional study) |
| 6 | Identification of dental calcification stages as a predictor of skeletal development phase [31] | Rebouças et al. (2021) | 113 panoramic, cephalometric, and hand-wrist radiographs | 9-15 years | Hispanic | Brazil | 53 males and 60 females | Observational study (Cross-sectional study) |
| 7 | Association between mandibular second molars calcification stages in the panoramic images and cervical vertebral maturity in the lateral cephalometric images [32] | Toodehzaeim et al. (2020) | 125 panoramic radiographs and lateral cephalograms | 8-17 years | Caucasian | Iran | 61 males and 64 females | Observational study (Cross-sectional study) |
| 8 | The correlation between dental stages and skeletal maturity stages [33] | Jourieh et al. (2021) | 295 panoramic and hand-wrist radiographs | 9-14 years | Caucasian | Syria | 145 males and 150 females | Observational study (Cross-sectional study) |
| 9 | Sensitivity and specificity of mandibular third molar calcification at chronological age and hand wrist maturation stage to discriminate between female and male at pubertal growth period [34] | Mardiati et al. (2021) | 423 panoramic radiographs and 423 hand-wrist radiographs | 8-17 years | Asian | Indonesia | 144 males and 279 females | Observational study (Cross-sectional study) |
| 10 | Evaluation of dental and skeletal maturity using digital panoramic radiographs and digital cephalograms [35] | Mustafa et al. (2015) | 60 digital panoramic radiographs, lateral cephalograms, and hand-wrist radiographs | 8-16 years | Caucasian | German | 45 males and 15 females | Observational study (Cross-sectional study) |
| 11 | Relationship between mandibular second molar calcification stages and cervical vertebrae maturity in Italian children and young adults [36] | Cossellu et al. (2014) | 500 panoramic radiographs and lateral cephalograms | 10-20 years | Caucasian | Italy | No data | Observational study (Cross-sectional study) |
| 12 | Skeletal maturity assessment using mandibular canine calcification stages [37] | Džemidžić et al. (2016) | 60 panoramic radiographs and lateral cephalograms | 9-16 years | Caucasian | Bosnia | 70 males and 81 females | Observational study (Cross-sectional study) |
| 13 | Use of the tooth coronal pulp index for recognition of the pubertal growth period [38] | Nawaya and Burhan (2016) | 262 panoramic and hand-wrist radiographs | 9-16 years | Caucasian | Syria | 125 males and 137 females | Observational study (Cross-sectional study) |
| 14 | Dental calcification stages as determinants of the peak growth period [39] | Litsas et al. (2016) | 255 lateral cephalometric and panoramic radiographs | 8-18 years | Caucasian | Greece | 110 males and 145 females | Observational study (Cross-sectional study) |
| 15 | Assessment of the pubertal growth period using the open apices of the lower teeth [40] | Issa et al. (2017) | 292 panoramic and 292 hand-wrist radiographs | 10-16 years | Caucasian | Syria | 150 males and 142 females | Observational study (Cross-sectional study) |
| 16 | Reliability of maxillary canine calcification stages and salivary alkaline phosphatase for pubertal growth prediction (cross-sectional study) [41] | Nasser et al. (2023) | 80 periapical radiographs of maxillary canine teeth, radiographs of the middle phalanx of the middle finger, and saliva samples | 8-16 years | Caucasian | Iraq | 43 males and 37 females | Observational study (Cross-sectional study) |
| 17 | Evaluation of the compatibility of C2, C3, and C4 fractal dimension values with hand-wrist and cervical vertebra maturation methods in determining skeletal maturation [42] | Pamukcu et al. (2022) | 120 lateral cephalometric and hand-wrist radiographs | 8-18 years | Caucasian | Turkey | 59 males and 61 females | Observational study (Cross-sectional study) |
| 18 | The relationship determination between menarche and the peak of skeletal maturation using hand wrist and cervical vertebrae index [43] | Mardiati et al. (2014) | 220 hand-wrist radiographs and lateral cephalograms, with 89 subjects having experienced menarche | 8-17 years | Asian | Indonesia | 220 females | Observational study (Cohort study) |
| No. | Author (Year) | Maturation Indicators | Comparison | Result | Conclusion |
|---|---|---|---|---|---|
| 1 | Firouzinia et al. (2022) [27] | Dental maturation (nolla) | Skeletal maturation (CVM) | There is a notable correlation between Cervical Vertebrae Maturation (CVM) and dental development. The calcification stages of teeth 13, 23, and 43 at stage 10 have reliable diagnostic value for predicting the post-puberty phase, while the calcification stages of teeth 17, 27, and 47 at stage 5 of dental development are useful for predicting the pre-puberty phase. | The diagnostic ability of the calcification stage of teeth to identify growth phase is limited; the calcification stage of teeth has a high diagnostic value in pre-puberty and post-puberty phases, but the calcification stage of the teeth is not reliable to detect puberty phase. |
| 2 | Sinha et al. (2016) [28] | Biomarker (IGF-1) | Skeletal maturation (CVM) | There was a significant positive correlation between serum Insulin-like Growth Factor-1 (IGF-1) levels and urine IGF-1 levels with Cervical Vertebrae Maturation Index (CVMI). Serum and urine IGF-1 concentrations demonstrated parallel variations throughout pubertal development and the aging process. | Urine IGF-1, along with serum IGF-1, is a promising indicator for growth assessment, potentially eliminating the need for radiographic evaluation. |
| 3 | Ojha et al. (2019) [29] | Dental maturation (Demirjian) | Skeletal maturation (hand-wrist) | The statistically significant correlation coefficients between skeletal maturation and dental calcification stages range from 0.61 to 0.88. The order of teeth based on the highest to lowest correlation for males is canine teeth, first premolar, second premolar, and second molar. The sequence in females is second molar, canine teeth, first premolar, and second premolar. | The stages of dental calcification can be utilized clinically as an indicator of maturation in the puberty growth period. |
| 4 | Günen Yılmaz et al. (2018) [13] | Dental maturation (Demirjian and Nolla) | Skeletal maturation (hand-wrist) | All teeth demonstrated a positive and statistically significant correlation, with the strongest correlation observed between the calcification stage of the mandibular second premolar and HWM. The highest correlation between the Nolla Method and the Demirjian method with skeletal maturation was found in 35 teeth. | The mandibular second premolar is the most accurate tooth for determining the pubertal growth stage based on both methods. |
| 5 | Mini et al. (2018) [30] | Dental maturation (Demirjian) | Skeletal maturation (CVM) | The correlation between dental maturation stages and Cervical Vertebrae Maturation Stages (CVMS) ranged from 0.61 to 0.74 for females and 0.48 to 0.69 for males. For both females and males, the second premolar teeth of the mandible have the highest correlation, and the canine teeth of the mandible have the lowest correlation. Stage G of the second premolar tooth of the mandible indicates the beginning of accelerated puberty growth in this study population. | Stage G of the mandibular second premolar can be used clinically as an indicator of maturation during the pubertal growth period. |
| 6 | Rebouças et al. (2021) [31] | Dental maturation (Demirjian) | Skeletal maturation (CVM and hand-wrist) | CVMI and second molar calcification are statistically significant predictors of Skeletal Maturation Indicators (SMI). The calcification stages E for males, and E and F for females, are associated with the phase before the peak of pubertal growth. Stages G and H in males, and stages F and G in females, align with the peak of pubertal growth. In the late maturation phase, most second molars exhibit closure of the root apices (stage H). | The calcification stage of the left mandibular second molar is considered a better predictor of maturation than the mandibular canine and can be used for early identification of the pubertal growth phase. |
| 7 | Toodehzaeim et al. (2020) [32] | Dental maturation (Demirjian) | Skeletal maturation (CVM) | There is a strong correlation between the calcification stage of the second molar calcification of the mandible and the growth stage. This stage of calcification of teeth only has diagnostic performance for post-puberty growth stage. A Likelihood Ratio (LHR) ≥10 is observed only in identifying the post-pubertal growth phase at stage H of the second molar. | The calcification stage of the mandibular second molar is a reliable indicator for estimating the optimal timing for treatment during the post-pubertal growth phase. However, it is not advisable for use in planning treatments that must commence during the pubertal or pre-pubertal growth phases. |
| 8 | Jourieh et al. (2021) [33] | Dental maturation (Demirjian) | Skeletal maturation (hand-wrist) | A statistically significant, strong positive correlation was observed. In males, the order from highest to lowest correlation was the second molar, second premolar, canine, and first premolar; whereas in females, it was the second molar, second premolar, first premolar, and canine. The second molar demonstrated the highest correlation in both sexes, while the first premolar showed the lowest correlation. | Tooth maturation stages can be utilized as dependable markers for assessing biological maturation, offering high diagnostic accuracy in identifying the pre-pubertal growth phase. |
| 9 | Mardiati et al. (2021) [34] | Dental maturation (Demirjian and Goldstein) | Skeletal maturation (hand-wrist) | A moderate correlation was found between the stages of the third molar in the mandible and chronological age, while the correlation between the third molar and HWM was low. At the HWM stage, the third molar calcification in the mandible showed high diagnostic accuracy. In women, at the S stage, sensitivity reached 97% with 100% specificity, while in men, at SMI-2, sensitivity was 94.5% and specificity was 99.99%. | Sensitivity and specificity in women and men suggest that the calcification of the third molar of the mandible is solely effective for diagnosing the pre-puberty growth phase. |
| 10 | Mustafa et al. (2015) [35] | Dental maturation (Demirjian) | Skeletal maturation (CVM and hand-wrist) | The relationship between skeletal maturation and the stage of dental maturation was statistically significant for boys and statistically insignificant for girls. Calcification stage of the second premolar teeth and second molar of the mandible in males showed the highest correlation. | Correlation between the stage of calcification of the teeth and indicators of skeletal maturation in boys may make it easier for doctors to identify the growth stage of puberty through panoramic radiography. |
| 11 | Cossellu et al. (2014) [36] | Dental maturation (Demirjian) | Skeletal maturation (CVM) | There was a good correlation between the second molar Demirjian Method and CVM index, both through Pearson (0.78-0.86) and Spearman (0.81-0.85) tests. | The mandibular second molar can serve as a reliable indicator for assessing the growth phase, but in women, the end of growth acceleration cannot be attributed to the stage of tooth maturation and should be considered alongside additional parameters, such as CVM, for a more comprehensive assessment. |
| 12 | Džemidžić et al. (2016) [37] | Dental maturation (Demirjian) | Skeletal maturation (CVM) | The correlation coefficient between the stage of calcification of mandibular canine teeth and skeletal maturation was 0.895 for males and 0.701 for females, and all correlation coefficients were statistically significant. | A significant correlation was observed between the calcification stage of mandibular canine teeth and skeletal maturation. However, the calcification stage of the mandibular canine was found to have acceptable diagnostic accuracy solely for assessing the prepubertal phase of growth. |
| 13 | Nawaya and Burhan (2016) [38] | Dental Maturation (coronal pulp index) | Skeletal maturation (hand-wrist) | No significant correlation was found between the Tooth Coronal Index (TCI) values of incisive teeth and canine teeth during the puberty growth period, while significant correlations were found for premolar and molar teeth. The highest correlation coefficient is found in the first and second molars. | The TCI for the mandibular first and second molars is the most significant during the pubertal growth period compared to other teeth. |
| 14 | Litsas et al. (2016) [39] | Dental maturation (Demirjian) | Skeletal maturation (CVM) | The relationship between the stages of skeletal and dental maturation was found to be statistically significant, stage E of the first premolar tooth showed the highest positive LHR to identify post puberty growth acceleration, while stage H of second molar tooth offered dependable diagnostic information to determine post puberty growth acceleration, and stage F of second molar tooth offered dependable diagnostic information to identify peak growth period. | The calcification stage of the second molar provides reliable diagnostic information to determine pubertal growth acceleration. |
| 15 | Issa et al. (2017) [40] | Dental Maturation (open apices) | Skeletal maturation (hand-wrist) | The correlation coefficient between SMI and the open apex value of each mandibular tooth was relatively high, ranging from 0.577 to 0.830, and statistically significant. The mandibular canine teeth exhibited the strongest correlation between SMI and their development, as evaluated using the open apex method. | Skeletal maturation is closely related to the measurement of open apexes in mandibular teeth. The beginning and end of puberty growth period can be predicted by measuring the open apex of the left mandibular canine tooth using panoramic radiography. This diagnostic method can be carried out without the need for hand-wrist radiography, thus minimizing radiation exposure during orthodontic treatment. |
| 16 | Nasser et al. (2023) [41] | Biomarker (ALP) | Skeletal maturation (MP3) and dental maturation (Demirjian) | Calcification stages of the upper jaw canine teeth are strongly correlated with skeletal maturation, and there is no significant correlation between skeletal maturation, the calcification stages of canine teeth, and Alkaline Phosphatase (ALP) levels. | Saliva ALP cannot be recommended as an indicator of maturation. In clinical practice, ALP levels in saliva cannot be used as a reliable indicator for detecting the proper phase of puberty. |
| 17 | Pamukcu et al. (2022) [42] | Skeletal maturation (fractal dimensions C2, C3, C4) | Skeletal maturation (CVM and hand-wrist) | No statistically significant correlation was found between fractal dimension values and the stages of CVM and HWM. A significant negative correlation was observed between the fractal dimensions of C4 and the HWM and CMV stages. | The value of the fractal dimension of C4 can serve as an objective tool for assessing skeletal maturation, particularly at puberty growth. |
| 18 | Mardiati et al. (2014) [43] | Sexual maturation (menarche) | Skeletal maturation (CVM and hand-wrist) | Menarche is linked to the maturation stages of both the hand-wrist and cervical vertebrae. It occurs 0.47 years after the MP3cap stage and 1.69 years after the CVMS2 stage, or 0.49 years before the CVMS3 stage. | Menarche can be used as an indicator to determine when the peak of puberty growth has passed and can also be used to predict the end of the puberty growth phase. |
4. DISCUSSION
Various methods can be used to assess growth, especially during the period of pubertal growth, including chronological age and physiological age, which include the stage of tooth development, mapping of height measurements, the stage of development of secondary sexual characteristics, and radiographic measurements of skeletal maturation [44]. In assessing pubertal growth using physiological maturation indicators, the HWM method is widely cited in various articles as the gold standard in assessing individual growth [45, 46]. CVM can also be the primary method in assessing pubertal growth due to the practicality of examination, which does not require additional radiography, thus preventing patients from receiving additional radiation [46, 47]. Studies suggest no significant difference in the reproducibility of HWM and CVM assessments of skeletal maturation. This means that both methods are considered adequate for clinical use by orthodontists [48]. However, to avoid overexposure to radiation and to use more practical methods, it is important to know the various alternatives for using maturation indicators to assess pubertal growth.
A total of 18 articles were reviewed in this study, and all of the articles used skeletal maturation as a comparison. There are 14 articles reviewing dental maturation indicators. Most articles that review dental maturation indicators use the Demirjian method, with a total of 11 articles. Other methods reviewed are Nolla, Goldstein, TCI, and Open Apices methods.
A total of 2 articles suggest that the second mandi-bular premolars have the highest accuracy [13, 30]. Günen et al. [13] stated that the second premolar of the mandible has the best prediction rate based on the Nolla and Demirjian methods and has the highest correlation with Hand-Wrist maturation stage. According to the Demirjian method, tooth 35 is the most significant tooth in detecting acceleration of pubertal growth. In addition, it is suggested that teeth 35, 34, and 33 in stage F and tooth 37 in stages E and F indicate the pre-peak stage of pubertal growth. Teeth 35 and 37 in stage G indicate the peak stage of pubertal growth, and teeth 35 and 37 in stage H indicate the post-peak stage of pubertal growth. Meanwhile, according to the Nolla method, the pre-peak stage of pubertal growth can be indicated by tooth 35 in the eighth mineralization phase, teeth 33 and 34 in the ninth mineralization phase, and tooth 37 in the seventh and eighth mineralization phases. The peak pubertal growth stage for tooth 35 is in the ninth mineralization phase, and the post-peak stage for teeth 35 and 37 is in the 10th mineralization phase. In this study, the results show no difference in terms of sex at the mineralization stage of tooth 35.
These findings are further supported by studies highlighting that stage G of the second mandibular premolar can be used clinically as an indicator of maturation during the pubertal growth period. The study suggests a correlation between the stages of dental maturation and CVM, ranging from 0.61 to 0.74 for women and 0.48 to 0.69 for men. For both women and men, second mandibular premolars have the highest correlation, at 0.74 and 0.69, respectively. Meanwhile, mandibular canine teeth have the lowest correlation, which is 0.61 for women and 0.48 for men [30].
In addition, the second mandibular molar teeth are also considered to have a high correlation with skeletal maturation in 4 articles [29, 31, 33, 39]. Rebouças et al. [31] found that the calcification stage of the second molars of the left mandible is better than the canines for assessing physiological maturation and can be used for early identification of the pubertal growth phase. The correlation between CVM and second molar calcification with SMI was considered statistically significant. The results revealed that the pre-peak phase of pubertal growth was at stage E of calcification for males and stages E and F for females. Stages G and H for males and stages F and G for females coincide with the growth peak. In the final growth phase, most second molars are at stage H.
Similarly, Jourieh et al. [33] found that second molars provide the highest correlation to skeletal maturation with the hand-wrist method for both males and females. The researchers stated that the order of correlation from highest to lowest was second molar, second premolar, canine, and first premolar in males, and second molar, second premolar, first premolar, and canine in females. The same result was stated by Litsas et al. [39], showing that the calcification stages of the second molar teeth provide good diagnostic information to determine the period of accelerated pubertal growth and have a statistically significant correlation with skeletal maturation. However, different results were presented by Ojha et al. [29], showing differences in the order of correlation in men and women. In men, canines have the highest correlation, followed by the first premolar, second premolar, and second molar. In contrast, second molars occupy the highest position in women, followed by canines, first premolars, and second premolars. Statistically, the correlation between skeletal maturation and the stages of tooth calcification ranges from 0.61 to 0.88 and is considered significant.
On the other hand, four articles show the limitations of using dental maturation indicators in assessing certain growth phases based on diagnostic performance [27, 32, 34, 37]. Firouzinia et al. [27] emphasized that Nolla's method is diagnostically effective in the prepubertal and post-pubertal phases, but less reliable during the pubertal phase. The results suggest that teeth 13, 23, and 43 in stage 10 of tooth calcification have an LHR+ above 10 for detecting the post-pubertal phase. Teeth 17, 27, and 47 in stage 5 of tooth calcification have an LHR+ above 10 to detect the prepubertal phase. However, the diagnostic ability of using the tooth calcification stage is not reliable for detecting the puberty phase. Similar results were revealed by Toodehzaeim et al. [32], stating that the Demirjian method for mandibular second molar calcification has diagnostic performance only in the post-pubertal growth phase, with an LHR value ≥10 for stage H in the second molar. Therefore, this method is not recommended for evaluating pubertal and prepubertal growth phases.
Other studies have similarly reported limitations associated with the use of dental maturation indicators in research. Džemidžić et al. [37] suggested a significant correlation between the mandibular canine tooth calcification stage and skeletal maturation. Still, the resulting performance is only satisfactory for the prepubertal phase. Meanwhile, a study by Mardiati et al. [34], used the Demirjian and Goldstein methods to assess the calcification of the third mandibular molar. The results show high sensitivity and specificity, but third molar calcification is only of high diagnostic value for the prepubertal growth phase.
Some studies also found differences in results between sexes, with a total of 2 articles. Both articles found a high correlation between dental and skeletal maturation in boys. However, in girls, according to Mustafa et al. [35], the correlation between dental maturation and skeletal maturation is considered low, while according to Cosellu et al. [36], at the end of the pubertal growth period for women, it cannot be linked to the stages of tooth maturation, thus requiring additional parameters such as CVM.
Another evaluated method was open apices. Research by Issa et al. [40] suggested that the measurement of the open apex of the left mandibular canine tooth has a high correlation with skeletal maturation, with a statistically significant correlation coefficient value. This method allows for the prediction of the beginning and end of the pubertal growth period without the need for additional radiography, thus reducing radiation exposure.
In addition, TCI was evaluated in another study, and the results stated that the first and second mandibular molars had the highest correlation coefficient during puberty compared to other teeth. However, TCI on the incisors and canines did not show a significant correlation in the pubertal growth period [38].
Based on the above review, the dental maturation indicator is proven to have a significant relationship with skeletal maturation in most of the articles that have been reviewed. Although the research results in various articles show differences, factors such as variations in the methods used, specific age groups, and sample sizes can influence these findings. In addition, several studies have reported limitations in the accuracy of this indicator at certain growth stages, as well as differences in correlation between males and females, highlighting the need for careful interpretation in its clinical application. However, the dental maturation indicator remains reliable due to its good correlation with skeletal maturation and practical assessment procedures, making it easier for operators to assess a patient's pubertal growth. Additional studies beyond the initial mapping have also supported this finding by reporting that dental maturation using the Demirjian method is a valid indicator for assessing pubertal growth. However, it cannot fully replace the HWM method [49]. A systematic review by Bruna et al. [50], further reinforces this by suggesting that dental maturation might serve as a potential indicator of skeletal craniofacial growth status.
In addition to dental maturation, various biomarkers have also been studied as indicators of physiological maturation to assess pubertal status. Biomarkers help predict the stage of skeletal maturation because bone growth and remodeling are controlled not only by local factors but also by systemic factors. The use of biomarkers to assess pubertal status helps reduce X-ray exposure. Biomarkers can be detected not only in serum but also in saliva. Biomarkers found in saliva and serum include IGF-1, Growth Hormone (GH), creatinine, and ALP [51]. Two research articles review the use of biomarkers in predicting pubertal growth.
IGF-1 is one of the most promising biomarkers. According to research by Sinha et al. [28], Serum IGF-1 and urinary IGF-1 levels show a significant positive correlation with CVMI and exhibit similar changes with pubertal growth and increasing age. This makes IGF-1, in both serum and urine, a potential alternative for assessing growth status without the need for radiographic assessment. However, different results were found for the ALP biomarker. One study stated that although the calcification stage of the upper jaw canine tooth correlates strongly with skeletal maturation, the correlation between skeletal maturation and salivary ALP levels is not significant. In clinical practice, salivary ALP cannot be recommended as a reliable indicator for accurately detecting the puberty phase [41]. This shows that ALP is not as accurate as IGF-1 and suggests that not all biological fluids can directly replace conventional methods for assessing pubertal growth. Overall, IGF-1 is more promising than salivary ALP in assessing skeletal maturation and can be an alternative for assessing pubertal growth without the need to use radiography. Despite these promising findings, limitations include a small sample size limited to female subjects, the absence of a longitudinal design, and the lack of validation against other maturity assessment methods. Additionally, potential biological and technical variability affecting IGF-1 levels was not extensively explored, highlighting the need for greater standardization in biomarker research to improve reliability and clinical applicability [28].
Supporting this finding, a systematic review by Dipak et al. [52] found that out of six saliva biomarkers, salivary IGF-1 emerged as a reliable indicator for skeletal maturity assessment. The current evidence from their review also suggests that salivary biomarkers may serve as an adjunctive tool for growth prediction during orthodontic treatment planning, alongside conventional assessment methods.
Another article reviews skeletal maturation by assessing fractal dimensions of C2, C3, and C4. The fractal dimension is a proposed indicator method for assessing skeletal maturation and its correlation with pubertal growth. The study by Pamukcu et al. [42], which reviewed fractal dimensions of the cervical vertebrae (C2, C3, and C4), reported inconclusive findings regarding their reliability. Overall, no statistically significant correlation was found between fractal dimensions and stages of skeletal maturation based on the CVM or HWM methods. On the other hand, a significant negative correlation was shown between the fractal dimension of the C4 vertebra and the stages of CVM and HWM. However, the results of the study show limitations in the use of this method.
Another maturation indicator reviewed in this study is the sexual maturation indicator. There is one article related to using sexual maturation indicators by reviewing menarche to assess pubertal growth. Mardiati et al. [43] state that menarche is closely correlated with the stage of skeletal maturation using the HWM and CVM methods. The research reports that menarche can be used to mark the peak of pubertal growth in individuals and to predict the end of the pubertal growth period. Although menarche can be used to assess pubertal growth well, it only applies to women, so it cannot be used to assess pubertal growth in men.
Alongside the effectiveness of the maturation indicators previously discussed, hormonal regulation has emerged as an important biological factor influencing bone develop-ment, thereby indirectly influencing the outcomes of orthodontic treatment. Adiponectin, for instance, plays a role in bone formation and holds promise in orthodontic applications. Erythropoietin, secreted by the kidneys, contributes to bone formation by increasing Vascular Endothelial Growth Factor (VEGF) expression. Estrogen also plays a key role in bone growth, bone maturation, and the regulation of bone turnover in adult bones [53]. It inhibits alveolar bone resorption by restraining osteoclastic differentiation and promoting osteoblast apoptosis. The effect of estrogen may attenuate the bone remodeling that occurs in Orthodontic Tooth Movement (OTM), thus limiting the rate of OTM [54]. This mechanism affects both fixed and removable orthodontic appliances. From a periodontal perspective, steroid hormones, especially estrogen, have a significant effect on gingival tissue and can increase the risk of periodontal disorders if oral hygiene is not maintained during orthodontic treatment. Compared to fixed appliances, aligners are kinder to periodontal tissues as they produce less plaque and inflammation, making them an optimal choice for cooperative and aesthetically concerned adult patients [55].
Moreover, in certain individual conditions, pubertal growth assessment may become unreliable, making standard maturation indicators less applicable. For instance, individuals with chronic diseases such as tuberculosis, treponemal infection, or rickets often experience delayed puberty that worsens with age [56]. Nutritional status also plays a major role. Obesity is frequently linked to earlier onset and faster progression of pubertal growth [57]. Genetic conditions such as Down syndrome are associated with slower growth rates compared to individuals without Down syndrome, but pubertal development in affected adolescents remains poorly understood [58]. These conditions disrupt pubertal growth patterns, limiting the accuracy of standard indicators in reflecting true maturation stages. Despite these limitations in specific populations, the predominant focus across the reviewed studies was on standard maturation indicators. Returning to the findings of the review, 77.8% discuss using dental maturation indicators [27, 29, 13, 30-40]. Among these articles, 57.1% show a significant correlation between dental and skeletal maturation, with the Demirjian method being dominant [29, 13, 30, 31, 33, 38-40]. This indicates that the dental maturation indicator can be the main alternative in assessing pubertal growth because it is supported by many research articles that suggest a significant correlation with skeletal maturation. Its high correlation makes dental maturation accurate for clinical practice and a relevant option for predicting pubertal growth without additional complicated diagnostic procedures. Meanwhile, 11.1% discuss using biomarkers, 50% of which show a significant correlation with skeletal maturation. As a result, the biomarker IGF-1 shows more significant potential than ALP as an indicator of maturation [28, 41]. Biomarker assessment, such as IGF-1, allows identification of puberty status without additional radiography, thus reducing radiation exposure to patients. These results make biomarkers a promising alternative method. In addition, 5.6% discuss fractal dimension assessment, which shows that the fractal dimension of cervical vertebrae has limited results, with a significant correlation only shown in the C4 vertebra [42]. Furthermore, 5.6% discuss sexual maturation by assessing individual menarche and its significant correlation with skeletal maturation [43].
Although this scoping review did not include a formal quality appraisal of the included studies, variations in methodological rigor were observed, particularly in study design, sample characteristics, and outcome measures. These differences may influence the strength and consistency of the reported findings and should be taken into account when interpreting the overall results.
Most of the included studies employed cross-sectional observational designs, which limit the ability to evaluate the progression of physiological maturation over time. This design constraint restricts the assessment of dynamic developmental changes and may reduce the precision in identifying the timing of pubertal growth stages. Additionally, the number of studies addressing sexual maturation indicators remains limited, highlighting the need for further empirical research to establish the validity and reliability of these indicators in the assessment of pubertal growth.
CONCLUSION
This review found that dental maturation is the most commonly used indicator and shows a strong correlation with skeletal maturation, making it a potential alternative for assessing pubertal growth. However, some studies noted limitations in its accuracy across certain growth stages and reported stronger correlations in males than females, indicating the need for cautious clinical interpretation. While dental maturation emerged as the most frequently applied and reliable indicator, some alternative methods, such as IGF-1 and menarche, also showed promising correlations and may complement clinical assessment where appropriate.
Despite the findings presented in this review, certain limitations should be acknowledged. Several studies included in the review focused on a limited age range, typically between 8 and 14 years, which may not fully represent the entire pubertal growth phase. Additionally, variations in population characteristics such as race, ethnicity, and nutritional status can influence the physiological maturation process. These factors may introduce bias and limit the generalizability of the findings across diverse populations.
AUTHORS’ CONTRIBUTIONS
The authors confirm their contributions to the paper as follows: Z.C.M., G.G., and E.S.: Study conception and design, data collection, analysis and interpretation of results, draft manuscript. All authors reviewed the results and approved the final version of the manuscript.
LIST OF ABBREVIATIONS
| CVM | = Cervical Vertebrae Maturation |
| IGF-1 | = Insulin-like Growth Factor-1 |
| CVMI | = Cervical Vertebrae Maturation Index |
| CVMS | = Cervical Vertebrae Maturation Stages |
| SMI | = Skeletal Maturation Indicators |
| LHR | = Likelihood Ratio |
| TCI | = Tooth Coronal Index |
| ALP | = Alkaline Phosphatase |
| HWM | = Hand-Wrist Maturation |
| GH | = Growth Hormone |
| VEGF | = Vascular Endothelial Growth Factor |
| OTM | = Orthodontic Tooth Movement |
AVAILABILITY OF DATA AND MATERIALS
The data supporting the findings of the article will be available from the corresponding author [Z.C.M] upon reasonable request.
ACKNOWLEDGEMENTS
Declared none.

